


The Underlying Truth "with" COVID-19 Mortality in Australia
Catching a case of COVID-19 mortality understanding

Late last year, the Australian Bureau of Statistics (ABS) released the “Causes of Death” data for the 2022 reference period.
The “key statistics” published on the ABS webpage showed how “COVID-19 caused 9,859 deaths and became the third leading cause [of death]”, pointing to just how rare this was by highlighting that an infectious disease was last in the top five leading causes of death in 1970.1
Naturally, this information was transmitted in the legacy media without critical analysis.2
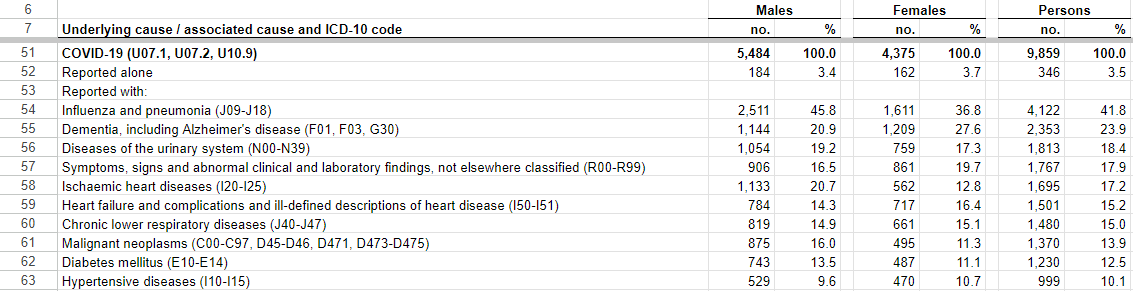
As it turns out, COVID-19 was reported as the “underlying cause of death” for just 346 of the 9,859 COVID-19 deaths in Australia in 2022 (see below):
So why were we told that COVID-19 was the third leading killer in 2022 in Australia?
The answer is a mixture of a “catch-all” measure of what constituted a COVID-19 fatality, dodgy data collection and reporting, and the failure of the COVID-19 vaccines.
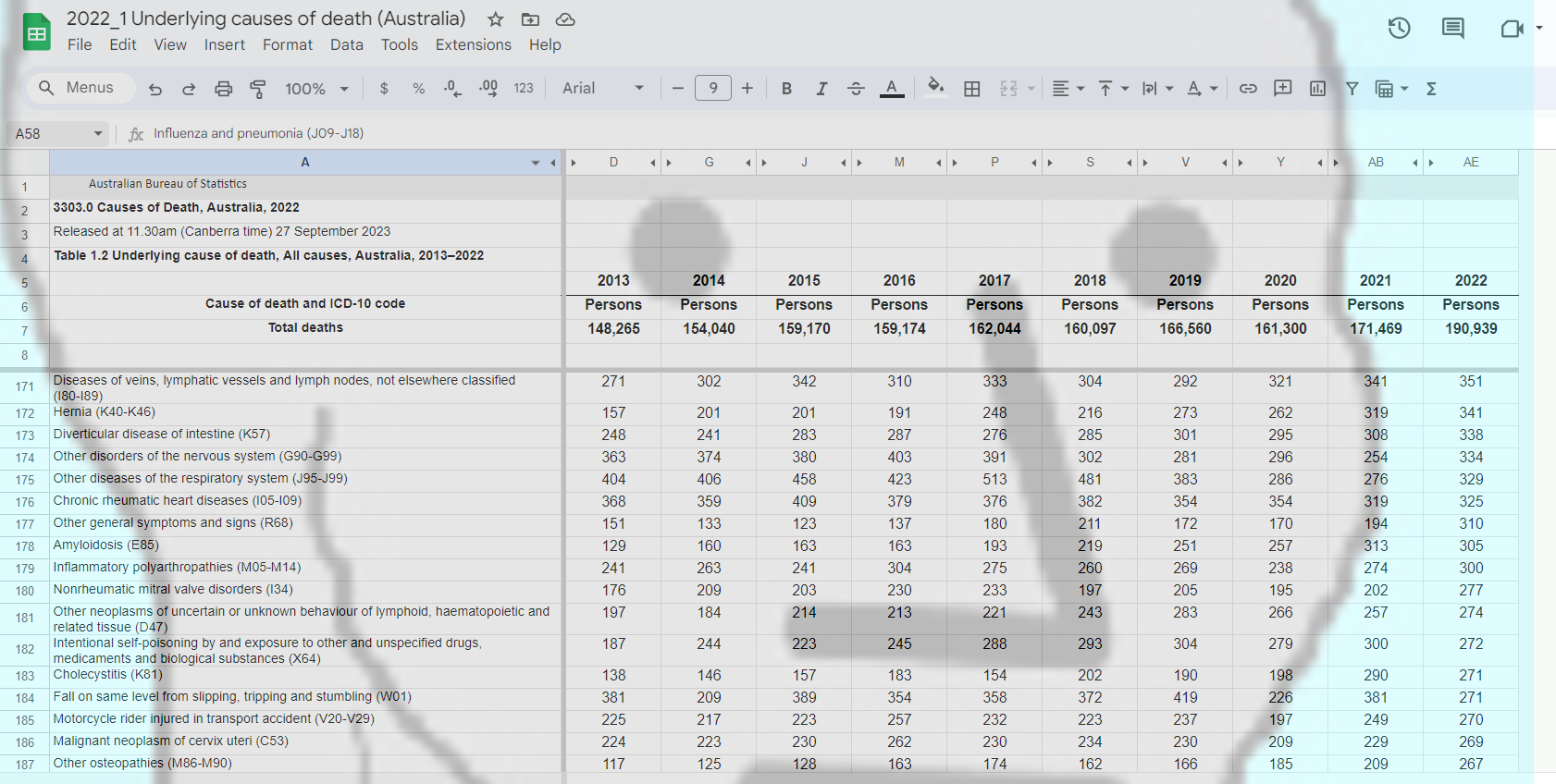
In this article we will analyse the World Health Organisation’s (WHO) guidance and how Australia’s largest state, New South Wales (NSW), applied such guidance in their COVID-19 data collection and reporting, showing how COVID-19 could be reported as Australia’s third-largest killer, but realistically, could have slotted in at about row 172 in 2022 in the “Causes of Death” release from the ABS:
The World Health Organisation (WHO) Guidance
In little over a month after the pandemic was declared, the World Health Organisation (WHO) issued guidance that a death should be reported as a COVID-19 death if it was:
“. . . a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma). There should be no period of complete recovery from COVID-19 between illness and death. A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19.”3 [emphasis added]
So, all that was required was a doctor or certifier to suspect COVID-19 was the culprit, when realistically any other respiratory illness such as pneumonia could have been the cause (reported with 41.8% of COVID-19 deaths in 2022). The WHO did not require doctors/certifiers to obtain a positive COVID-19 test to complete a death certificate stating one had died of COVID-19.
In circumstances where a positive test result prior to or following a person’s death could be obtained, we have reason to be sceptical of what a positive PCR test could show. During the COVID-19 pandemic in Australia, we know that higher Ct values (35-45 cycles) were used which could have led to the detection of fragments of the virus (even in samples from individuals with a low viral load or who have already recovered from the infection), resulting in false positives.4
The WHO guidance also suggested that if someone died and COVID-19 was “involved” (confirmed or probable remember?), their death should be recorded as a “COVID-19 death”, regardless of any preexisting conditions they might have had. Even if those conditions might have worsened their reaction to COVID-19, the death should still have been attributed to COVID-19, not to the preexisting condition like cancer, ischaemic heart disease, dementia or diseases of the urinary system - some of the most commonly reported “with” COVID-19 deaths from 2022 in Australia. It is likely, therefore, that many of Australia’s 9000+ COVID-19 deaths were wrapped up with other causes as the “Multiple Causes of Death” data (shown above) reveals.
This broad definition could even have meant that, hypothetically, someone who suffered and died from the conveniently ubiquitous condition we know as “Long COVID” could be recorded as a “COVID-19 death” because they had not had a “period of complete recovery . . . between illness and death”.
In a pandemic scenario, this broad definition was likely to have been implemented to serve a broad purpose called the “manipulative conception of causality”. It is argued, that in a pandemic scenario, the guiding principle is to choose an underlying cause of death that is dictated by public health and epidemiological concerns.
In priming the pandemic, experts created the fear that SARS-CoV-2 was a pathogen that required the most extreme public health interventions, even if that required calling all clinically-compatible illnesses COVID-19 deaths as a preventative measure so that interventions could be designed to prevent the worst from possibly occurring.
Previously, the WHO had deployed a similar strategy regarding HIV, attributing all causes of death which were ill-defined or unknown (including many others) as “HIV positive”. As in the case of COVID-19, this was supposed to reflect interests of importance for public health, rather than what was acceptable from a purely medical point of view. This resulted, however, in a far greater number of conditions being coded as HIV-related than before, just as today, with this strategy for COVID-19 death reporting, we have grossly inflated figures regarding COVID-19 deaths.5
It is a perfect example of circular reasoning:
Pandemic because high number of cases;
Because pandemic, change mortality data reporting to catch all suspected COVID cases (to benefit public health of course!);
New mortality data shows COVID-19 is killing extraordinary numbers of people;
Therefore, pandemic!
Dodgy “deaths” data collection and reporting
Although the criteria for certifying COVID-19 as an underlying cause of death was sufficiently broad to ramp up the fear and panic about COVID-19’s lethality, NSW Health took it one step further.
As it turns out, a “COVID-19 death” was not even required to be caused by COVID-19 to have been reported so:
“For 2020 through 2021, NSW Health categorised deaths as COVID-19 deaths if they met the definition in Communicable Diseases Network of Australia’s (CDNA) COVID-19 National Guidelines for Public Health Units. As per the CDNA definition, deaths were considered COVID-19 deaths for surveillance purposes if the person died with COVID-19, not necessarily because COVID-19 was the cause of death.”6 [emphasis added]
It appears that NSW Health took some liberties with the CDNA definition which actually stated:
“A COVID-19 death is defined for surveillance purposes as a death in a confirmed or probable COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID-19”7 [emphasis added]
The CDNA's definition suggested that a death should have been recorded as a COVID-19 death if there was no clear, unrelated cause of death. This implied that COVID-19 should have been a significant factor or contributing factor in the death.
By NSW Health's interpretation, however, if the person died with COVID-19, not necessarily because of it, their approach would have included cases where COVID-19 was present, but not the primary cause of death.
Dodgy “hospitalisations” data collection and reporting
Similarly, the loosest of criteria were used for categorising “COVID-19 hospitalisations” during the pandemic.
In an admission that has to be watched to be believed, a NSW Health spokesperson explained that because of their “back-capture” processes, COVID-19 “hospitalisations” had been significantly overestimated.
In this 11 February, 2022 press conference, NSW Health provided the hypothetical example of a COVID-19 “hospitalisation”:
22 year old male, recovered from COVID-19 infection three weeks ago, goes bike riding, breaks his arm, attends hospital, recorded as a “COVID-19 hospitalisation”
Source: NSW Health Press Conference, 11 February 2022
So, not only were all “hospitalised” COVID-19 patients not admitted because of COVID-19, but that these patients could have even recovered from COVID-19 up to 28 days prior to admission to hospital.
The evidence presented here raises serious questions about the completeness and accuracy of the COVID-19 data we have been fed since the pandemic commenced.
Conclusions
Why was COVID-19 Australia’s third largest killer in 2022?
We have learned that the WHO definition was so broad that it could encompass all respiratory deaths, resulting in having them coded as “COVID-19 deaths”.
Undeniably, the virus was rampant in Australia from the end of 2021 and in 2022 and so, detecting the virus was not a problem for doctors and certifiers responsible for mortality reporting at the time, however, as touched on in a previous article, it seems that the medical establishment somehow forgot how to treat pneumonia resulting in many more deaths “with” COVID-19 in 2022 than there otherwise should have been (41.8% of COVID-19 deaths were reported with pneumonia).
But, thinking about it again, why exactly did the virus run rampant in a 95% mRNA “fully vaccinated” country? After all, the promised “roadmap to freedom” and path out of the pandemic was through vaccination was it not?
Yet vaccination, in particular third-dose booster vaccination, corresponded with surges in excess mortality in Australia in 2022, and the third-leading cause of death driving this excess mortality, we are led to believe, was COVID-19:
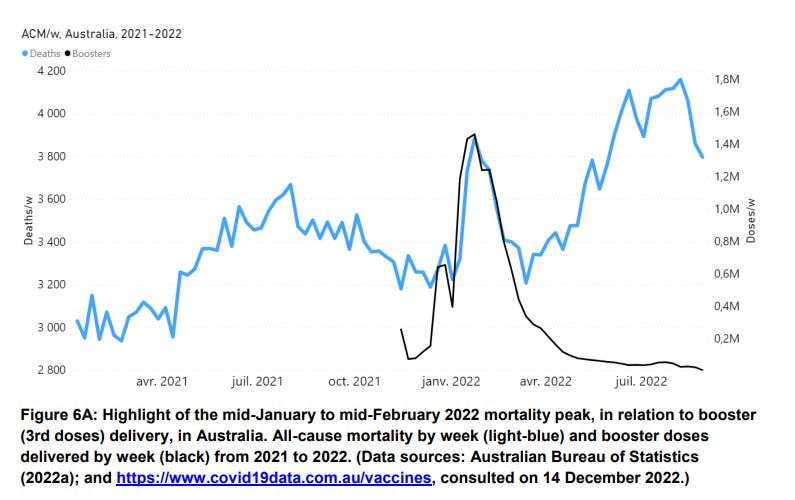
Note how in the above graph, the booster doses (black line) given predate the surges in deaths (blue line) confirming the hypothesis held by many, and explored in our articles previously, that serious harms from COVID-19 vaccination, resulting in death, have occurred.
These deaths could then be recorded as “COVID-19 deaths” because they were “clinically compatible” to COVID-19 (such as pneumonia), or could be associated with cardiovascular mortality (experts always assure us that COVID-19 infection is a far more likely culprit than from any “rare”, “mild” or “transient” side effect from vaccination) or simply could be bundled with the “unknown deaths” that continue to baffle the experts.
In this way, COVID-19 could be recorded as Australia’s third-largest killer in 2022, it just gives us very little insight into what had actually caused and continues to cause the absolute carnage that no one seems to be at all remotely interested in investigating, or even acknowledging.
Australian Bureau of Statistics (2022), Causes of Death, Australia, ABS Website, accessed 4 October 2023.
Take your pick from this sample of Google News search results using the term “COVID third leading cause of death Australia”, search conducted 4 October 2023 (archived here)
World Health Organisation, “International Guidelines for Certification and Classification (Coding) of COVID-19 as a Cause of Death”, 16 April 2020, p. 3, archive link, accessed 5 October 2023.
The presumed “gold-standard” PCR test (reverse transcriptase polymerase chain reaction) for detecting COVID-19 involves amplifying the genetic material through a series of cycles. Cycle thresholds (Ct) play a significant role in determining the presence and quantity of genetic material from a virus in a sample from . A lower Ct value indicates that the virus's genetic material was detected at an earlier stage, suggesting a higher viral load in the sample. Conversely, a higher Ct value suggests a lower initial viral load. The variability in cycle thresholds (CT) during the PCR testing process for COVID-19 will have led to varying results, potentially yielding false positives due to differences in viral load amplification.
Amoretti, M. C., & Lalumera, E., “COVID-19 As the Underlying Cause of Death: Disentangling Facts and Values ”, History and Philosophy of the Life Sciences, 43(1), 4, 2021. https://doi.org/10.1007/s40656-020-00355-6
NSW Health, “COVID-19 Surveillance Report Data Sources and Methodology”, https://www.health.nsw.gov.au/Infectious/covid-19/Pages/surveillance.aspx, accessed 25 January 2024.
CDNA, “Coronavirus Disease 2019 (COVID-19) CDNA National Guidelines for Public Health Units”, https://www.health.gov.au/sites/default/files/documents/2022/10/coronavirus-covid-19-cdna-national-guidelines-for-public-health-units.pdf, accessed 25 January 2024.
While the manufactured hysteria has now died down, the laws and measures introduced during the “lockdowns” remain on the books, and the camps are quietly maintained, available for use when the time comes.
Thank you for your articles. Particularly on Australia Day, it is fitting to reflect on our birth right and to remain vigilant that this nonsense does not recur.