
The Startling Increase of Deaths by Unknown Causes in Australia
The rise of deaths by unknown causes in the period 2019-2021 in Australia

Since the rollout of the COVID-19 vaccines, there has been a proliferation of stories in the media involving people who “died suddenly”. The evidence of this surge in “sudden deaths” has been accompanied by a similar rise in “unknown deaths”; those categorised as “Other ill-defined and unspecified causes of mortality (International Classification of Diseases Version 10 [ICD-10] code R99)” in the ABS “Causes of Death” (COD) release.1
Since 2019, deaths from ICD-10 code R99 have risen from an average of 790 deaths per year in the period 2012-2018 to a total of 2,366 deaths in 2021:

In this article, we investigate the reasons for this substantial increase in “unknown deaths” in Australia since 2019.
Changes in reporting by the ABS
The increase in “unknown”, R99 deaths, is partly a result of a change in reporting adopted by the ABS in 2015 for its mortality reports.
The ABS used to release its annual COD dataset 15 months after the end of each reference period. From 2015 onwards, however, it has been released 6 months earlier, representing a significant change in processing of the national mortality dataset.2 The result of the reporting change has been that that, at the time of reporting, more coroner-referred cases have not been finalised and are therefore, added to “revisions” in subsequent COD reports.3 For example, in preliminary reporting, there were 1,747 R99 deaths in 2019 (1,498 of which were coroner-referred deaths) which were finalised and reduced to 1,239 R99 deaths in the 2021 COD report: a 29.1% decrease.4 Based on this trend, we expect R99 deaths to decrease in subsequent COD reports as specific causes of death will be identified.5
It is estimated that the reduction in R99 deaths resulting from these revisions, however, will not fully offset the substantial increase in R99 deaths observed. Noting that the 1,239 deaths in this category in the finalised 2019 data is still well beyond the approximate 800 deaths expected based on historical trends. Despite revisions to data in years following the COD release, a large quantity of deaths which are categorised as “unknown” R99 deaths remain.6
The change in reporting adopted by the ABS in 2015 explains the rise in “unknown deaths” in Australia, but it explains neither the scale of the increase, nor why they have persisted upon the completion of the mortality data revisions process. In subsequent reports we will learn more about why more Australians are dying suddenly as either these deaths will be recategorised with different ICD-10 codes, or we will simply have to accept that more Australians are dying of “unknown causes”.7
Therefore, the change in reporting adopted by the ABS in 2015 does not fully account for the substantial increase in R99 deaths observed and other factors must be considered.
Is it the disappearance of deaths by cardiac arrest?
The increase in R99 deaths might also be partly explained by the disappearance of cardiac arrest deaths since 2019:
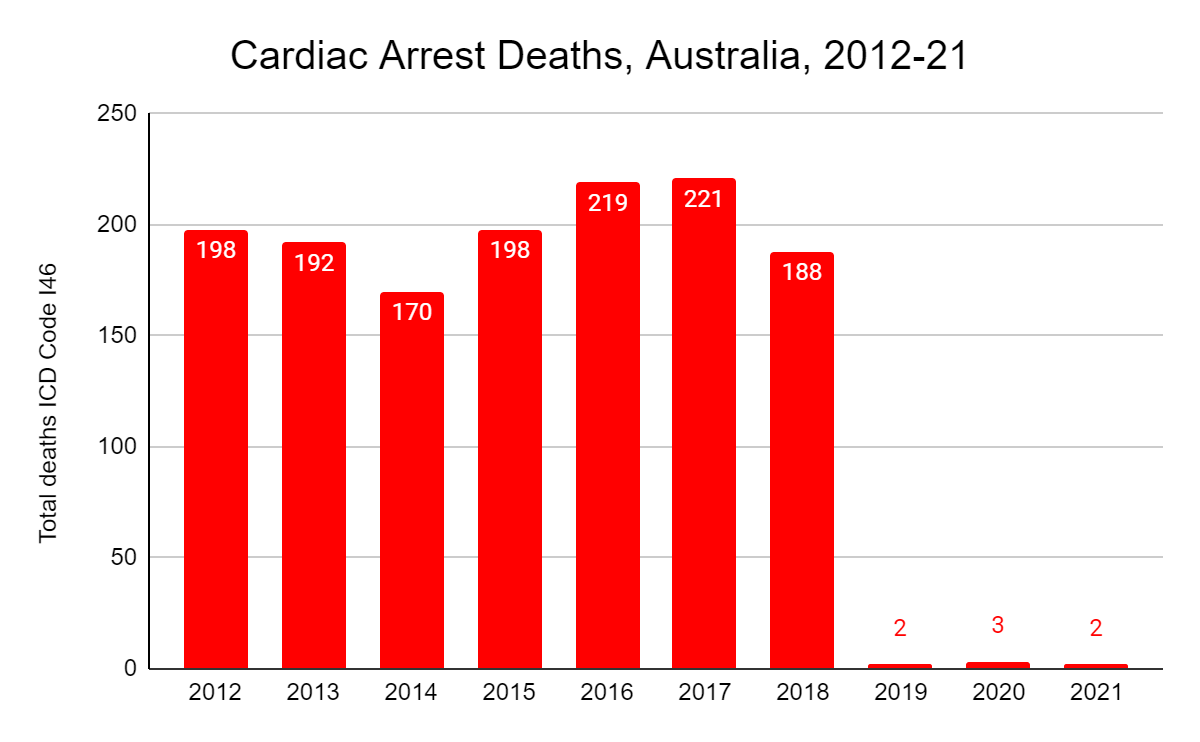
In the period 2012-2018, cardiac arrest deaths averaged about 200 per year in Australia, and in the majority of these cases, cardiac arrest was reported alone as the underlying cause of death with few other causes reported. Therefore, in usual circumstances we would expect approximately 200 deaths reported as “cardiac arrest” each year.
Far from being a medical miracle in Australia though, since 2019, deaths by the underlying cause of “cardiac arrest” (ICD-10 code I46) have been categorised as code R99 following guidance from the World Health Organisation (WHO):
“Not to be used for underlying-cause mortality coding. If no other cause of death is reported, code R99.”*8
*In relation to ICD-10 code I46.9 “Cardiac arrest, cause unspecified”
Since its recommended implementation in 2019, the ABS has confirmed that they have followed this guidance and the evidence, of course, confirms this change.
The disappearance of cardiac arrest deaths as a separate category raises questions about the accuracy of mortality data. It is unclear why death by cardiac arrest is no longer considered a valid underlying cause, especially if deaths such as these are moved out of a specific category and into a general one such as R99. The change in reporting will result in many cardiac related deaths from 2019 onwards remaining as R99 deaths, even once coronial investigations are concluded.
The reclassification of deaths attributed to cardiac arrest has contributed to the upsurge in fatalities falling under the R99 category, however, we should expect that those deaths categorised R99 to have increased by approximately 200 each year based on historical averages of deaths by cardiac arrest.
As deaths by this cause have increased substantially more than the addition of the “expected” annual cardiac deaths, additional factors or causes may be contributing to the rise in R99 deaths.
Is it “SADS”?
A relatively new term that has appeared to explain the voluminous reports of healthy and often young adults dying is “Sudden Adult Death Syndrome”, or more correctly, “Sudden Arrhythmic Death Syndrome” (SADS). SADS describes a group of rare heart conditions that can cause sudden cardiac arrest or death, usually in young and seemingly healthy individuals.9 These conditions are typically associated with abnormalities in the heart's electrical system and can lead to irregular heart rhythms, or arrhythmias.
We are told there’s “nothing new about SADS” and claims that these had increased were “baseless”.10
Indeed, the evidence from the ABS mortality reports seems to support this assertion. Deaths by ICD-10 code I49 “Other Cardiac Arrhythmias” have been largely consistent over the course of the last decade:

Similarly, deaths categorised “Other Sudden Death, Cause Unknown” (ICD-10 code R96) have barely registered a blip in this same period:

Therefore, it is not evident, from the presently available data, that reported increases in SADS deaths are contributing to a rise in I49 or R96 deaths, yet they could be leading to the increase in R99 deaths.
Supporting this hypothesis is the likelihood that many SADS deaths, given their sudden nature, will have ongoing coronial investigations which will contribute to the surge in R99 deaths observed in 2020 and 2021. It is unclear how many of these coronial investigations will yield insights as to the underlying cause of death, or whether they will remain in this “unknown” category once the investigations conclude and the data is finalised. Based on the percentage reduction in R99 deaths in 2019 (the first year of excess R99 deaths with finalised data) , one might reasonably expect that approximately only 30% of these deaths will be recategorised as deaths from other underlying causes.
In sum, it is expected that the majority of the R99 deaths in 2020 and 2021 will remain “unknown” following the completion of coronial investigations and the finalising of mortality data. The increase for 2019-2021 is larger than trends from 2012-2018, therefore, other factors for this increase in R99 deaths must be considered.
Is it the “vaccines”?
The surge in excess mortality observed in countries with high COVID-19 vaccination rates indicates a potential link between COVID-19 vaccination, the rise in deaths classified as “sudden” and the increase in R99 deaths in Australia in 2021.11 The hypothesis is supported by emerging evidence which demonstrate a causal link between sudden cardiac death (SCD) and COVID-19 vaccination, particularly in people under the age of 45 years:12
In a South Korean study, researchers conducted a comprehensive nationwide study on the incidence and outcomes of COVID-19 vaccination-related myocarditis (VRM). In their research, they found 21 deaths from vaccine-related myocarditis. Eight out of 21 deaths were SCD attributable to VRM proved by an autopsy, and all cases of SCD attributable to VRM were aged under 45 years and received mRNA vaccines.13 The researchers concluded “vaccine-related myocarditis was the only possible cause of death” in all of these cases of death.14
In a Japanese study, researchers examined autopsy findings from people who had died within 7 days of COVID-19 vaccination in Tokyo Metropolis. In five of the 54 autopsies, a “possible” causal link between COVID-19 vaccination and the cause of death was identified. Despite the mean age of the deceased individuals in the study (68.1 years) significantly exceeding the higher-risk age groups (young males) for vaccine-related myocarditis, and therefore, potentially minimising the likelihood of finding VRM, deaths in those aged over 45 of VRM were also observed, along with other causes of death linked with COVID-19 vaccines such as “cerebral haemorrhage”. In this study, only four of the cases were aged <45, yet in this small sample, two of these individuals died of VRM, and one - which resembles the Australian experience - of “unknown causes”.
In a Qatari study, researchers examined every death occurring within 30 days of COVID-19 vaccination in Qatar between January 2021 and June 2022. In the study period, 56 deaths were recorded after one dose, 65 deaths after two doses and 17 deaths after three doses. Of the combined 138 deaths, eight deaths were classified as “having high probability of being related to vaccination”; all of which were sudden cardiac deaths in persons with “no known risk factors for cardiac disease”. Of the 138 deaths, 52 were assigned a probability of being related to COVID-19 vaccination ranging from high-low probability. In 40 of these 52 cases, the causes of death was “sudden cardiac death”.15
In a German study, researchers examined autopsy findings from people who had died within 20 days of vaccination, confirming that five of 35 in the study had died within seven days of vaccination from causes consistent with vaccine injury. For four of the deceased, it was their first dose: and one occurred within 12 hours of vaccination.16
Similar results were summarised in a systematic search for English case-reports of cardiac complications of COVID-19 vaccines. Researchers concluded the “overall rate of post-COVID19 vaccination-myocarditis is around 1.62%” per injection.17 We note that not all cases of myocarditis are fatal, but equally, not all are “mild” as demonstrated in the South Korean study, and on the evidence presented in this systematic search, nor are they “rare”.
Most damning of all is a preprint published 5 July 2023 titled “A Systematic Review of Autopsy Findings in Deaths after COVID-19 Vaccination”. In this study, researchers investigated possible causal links between COVID-19 vaccine administration and death using autopsies and post-mortem analysis. The researchers screened PubMed and ScienceDirect for all published autopsy and necropsy reports relating to COVID-19 vaccination through May 18th, 2023 using keywords relating to COVID-19 vaccines, death, autopsy, and necropsy, returning results for 44 papers, covering 325 autopsy cases. Three physicians independently reviewed all deaths and determined whether COVID-19 vaccination was the direct cause or contributed significantly to death. The physicians confirmed a total of 240 deaths (73.9%) were directly due to or significantly contributed to by COVID-19 vaccination.18
These are but of few of the examples from emerging research that demonstrate a causal link between COVID-19 vaccination and severe adverse events including death which could explain the rise in unknown deaths in Australia. The above studies rely mostly on autopsy studies which provide more comprehensive information about the deceased, but with a much smaller sample size.
A much more comprehensive sample size we could use to confirm the hypothesis that vaccines have caused this surge in R99 deaths in Australia is derived from a dataset held by the ABS called “AIRMADIP” (“The “Australian Immunisation Register Multi-Agency Data Integration Project”). AIRMADIP links data from Australia’s national vaccination register with information on Australians’ health, education, government payments, income and taxation, employment, and population demographics: including deaths. AIRMADIP could be used to investigate vaccine information with mortality data such as:
The vaccination status of the deceased (unvaccinated, single, or many dosed);
The vaccine types administered to the deceased (viral vector or mRNA or mixed);
The vaccine batch(es) administered to the deceased;
The timing of vaccines given to the deceased;
The cause(s) of death of the deceased;
The industry in which the deceased was employed (were they subject to vaccination mandates?)
In November 2022, the “Australian Statistician” (the “Agency Head of the ABS”), David Gruen OA19, assured Australians that access to this dataset was available.
At Senate Estimates for the Economics Legislation Committee of the Australian Federal Parliament, Gruen was interrogated by Australian Senator Gerard Rennick about whether the ABS was tracking the concerning levels of excess mortality in Australia and importantly, the vaccination status of those who had died.
In reply, Gruen had this to say:
“In terms of tracking the vaccination status, that would require an analysis of microdata which is available. The Australian Immunisation Register has been linked to an integrated data asset that goes by the name of MADIP, which is a people-centred integrated data asset. It would be possible for a researcher to examine that. That would be possible.”20
The exchange is shown below (a tidied, edited extract of the exchange has also been posted to the Parliament of Australia page too):
Despite promises of access to this dataset, however, access to AIRMADIP has proved exceedingly difficult to obtain. Even Senator Rennick had not been provided access as of late April 2023.21
AIRMADIP is “gatekept” by the ABS in a “privacy by design approach” limiting its access to “approved researchers”. To date, it appears that only one group of researchers has made use of this dataset, and they have not used the information to show the absolute safety nor effectiveness of COVID-19 vaccines.22
We are aware of many others who have been ignored or denied access to AIRMADIP.
By utilising AIRMADIP, we could potentially provide compelling evidence supporting the unequivocal safety and effectiveness of COVID-19 vaccination. We could show that the unvaccinated had proportionally far worse mortality outcomes than the many-vaccinated.
So why is it not being used to do so?
Why is access to AIRMADIP so hard to secure?
We suspect that the evidence from AIRMADIP does not support the “safe and effective” propaganda.
Conclusions
In this article, we have demonstrated evidence of a substantial increase in “unknown deaths” in Australia during the period from 2019-2021. The increase is neither explained by changes in mortality reporting, nor the recategorisation of cardiac arrest deaths as R99 deaths.
It is estimated that revisions to mortality data will not reduce the number of “unknown deaths” to expected trend levels once data finalisation by the ABS is concluded.
We expect that the reported rise in SADS deaths are contributing to a rise in unknown deaths, and that it is possible that the majority will remain “unknown” once coronial investigations are concluded.
We suspect that fatal adverse reactions to COVID-19 vaccination are likely to have contributed to R99 deaths in 2021, however, the extent to which will be confirmed with future revisions to mortality data. The rise in unknown deaths is not explained by fatal adverse reactions to COVID-19 in 2019 and 2020, as the rise in R99 deaths preceded the rollout of Australia’s COVID-19 vaccination program in February 2021.
We estimate that the R99 deaths will significantly increase in 2022, corresponding with the record excess mortality in this year in Australia.
Finally, we suspect that many SADS deaths have been improperly categorised as “COVID-19 deaths”, however, we will explore the evidence supporting this last hypothesis in the next article. Furthermore, we will explore the decline in the rates of autopsies which might explain this increase in unknown deaths in Australia.
The Paradigm of the safety and effectiveness of COVID-19 vaccination is difficult to shift in the minds of the cognitively dissonant who would rather assure themselves that the pandemic was a threat but it is no longer; even now with excess mortality soaring and COVID-19 deaths remaining higher than at any point during the first years of the pandemic. Lockdowns of entire healthy populations to stop the spread of a respiratory pathogen that only ever threatened the old and sick have been rationalised as “doing the best we could” with little acknowledgement of the severity of the ongoing socioeconomic carnage caused. There is a lot at stake as the authors of the paper “A Systematic Review of Autopsy Findings in Deaths after COVID-19 Vaccination” conclude:
“If the alarmingly high number of reported deaths are indeed causally linked to COVID-19 vaccination, the implications could be immense, including: the complete withdrawal of all COVID19 vaccines from the global market, suspension of all remaining COVID-19 vaccine mandates and passports, loss of public trust in government and medical institutions, investigations and inquiries into the censorship, silencing and persecution of doctors and scientists who raised these concerns, and compensation for those who were harmed as a result of the administration of COVID-19 vaccines.”23
The preprint, quoted above, has since been removed from The Lancet in an overt act of censorship (which other counter-narrative academics have experienced).
Big Tech’s “results are changing quickly”, suggesting efforts are being made to scrub the paper from the Internet.
At least the paper was viewed 28,550 times, and hopefully the Streisand Effect yields many more.
The Paradigm will shift, though it might take longer than we had hoped.
The ABS applies these codes to deaths following guidance from the World Health Organisation’s International Classification of Diseases 10th Revision (ICD-10 Codes).
Australian Bureau of Statistics, “Causes of Death, Australia Methodology”, link here, accessed 1 July 2023.
“Data are deemed preliminary when first published, revised when published the following year and final when published after a second year.” Ibid., accessed 4 July 2023.
Ibid., link here. Interestingly, there appears to have been no change in the total R99 deaths in Table 1.2 of the ABS COD release from 2019 to 2020 despite the revisions process. Comment has been sought from the ABS for the discrepancy.
We note here that the ABS has repeatedly affirmed that 2020 was a “low mortality year”, justifying its exclusion from “baseline average” calculations of mortality and so, the large increase in R99 deaths in 2020 is even more significant.
“Doctors are baffled” might have been a similar way of expressing this idea, but we did not want to detract from the seriousness of the tone of the article. We note here that the potential recategorisation of R99 deaths may contribute to increases in other categories of causes of death, for example, “diseases of the circulatory system”; hypothetically raising the possibility of even greater excess mortality in these specific categories of death than those already addressed in a prior article here.
World Health Organisation, “Official WHO Updates Combined 2015-2017 Volume 2”, page 31, link here, accessed 2 July 2023.
Royal Australian College of General Practitioners, “Sudden Arrhythmic Death Syndrome”, link here, accessed 3 July 2023.
Australian Associated Press, “There’s nothing new about sudden adult death syndrome”, https://www.aap.com.au/factcheck/theres-nothing-new-about-sudden-adult-death-syndrome/, accessed 6 July 2023.
Australia’s COVID-19 vaccines were first approved for use in February 2021, and therefore, the surge in R99 deaths in 2019 and 2020 are not explained by the COVID-19 vaccines.
South Korean Paper - Jae Yeong Cho and others, “COVID-19 Vaccination-Related Myocarditis: a Korean Nationwide Study”, European Heart Journal, Volume 44, Issue 24, 21 June 2023, Pages 2234–2243, https://doi.org/10.1093/eurheartj/ehad339.
Japanese Paper - Suzuki, H., Ro, A., Takada, A., Saito, K. and Hayashi, K., “Autopsy Findings of Post-COVID-19 Vaccination Deaths in Tokyo Metropolis, Japan, 2021”, Legal Medicine, Volume 59, 2022, https://doi.org/10.1016/j.legalmed.2022.102134.
Qatari Paper - Butt, AA., Guerrero, MD., Canlas, EB., Al-Dwairi, H., Alimam, ABMA., Mohamad, AR., Ali, MT., Asaad, NA., Alkeldi, AASS., Mohammad, MFS., Thomas, AG., Al-Khal, A., Al-Maslamani, M., Abou-Samra, AB., “Evaluation of Mortality Attributable to SARS-CoV-2 Vaccine Administration Using National Level Data from Qatar”, Nature Communications, 2023 January, 3;14(1):24. https://doi:10.1038/s41467-022-35653-z.
German Paper - Schwab, C., Domke, L.M., Hartmann, L. et al., “Autopsy-Based Histopathological Characterization of Myocarditis after Anti-SARS-CoV-2-Vaccination”, Clinical Research in Cardiology, 112, 431–440 (2023). https://doi.org/10.1007/s00392-022-02129-5
The attribution of these eight additional deaths to VRM was only made after autopsies were conducted: the deceased had not shown clinical signs of VRM prior to death. It raises the question, how many other cases of sudden cardiac death without autopsy might we miss?
Jae Yeong Cho and others, op. cit., p. 2242.
Butt, AA. et. al., op. cit., p. 2.
Schwab, C., op. cit., p. 434.
Paknahad, MH., Yancheshmeh, FB., Soleimani, A., “Cardiovascular Complications of COVID-19 Vaccines: A Review of Case-Report and Case-Series Studies”, Heart and Lung. 2023 May-Jun; 59, p. 174.
Hulscher, N., Alexander, PE., Amerling, R., Gessling, H., Hodkinson, R., Makis, W., Risch, HA., Trozzi, M., McCullough, PA., “A Systematic Review of Autopsy Findings in Deaths after COVID-19 Vaccination”, https://ssrn.com/abstract=4496137, accessed 5 July 2023: UPDATE: the preprint at the above link was removed 7 July 2023. At present (7 July 2023), it can be downloaded here https://zenodo.org/record/8120771 and I have a downloaded copy if you need one, please ask via email, or in the comments.
“Order of Australia”: The Order of Australia is an honour that recognises Australian citizens and other persons for outstanding achievement and service. It was established on 14 February 1975 by Elizabeth II, Queen of Australia, on the advice of the Australian Government.
Commonwealth of Australia, “Senate Economics Legislation Committee - Estimates”, link here, page 25.
Confirmed via email exchange with Senator Rennick, 26 April 2023.
The publication on the page is entitled “Socioeconomic Determinants of Vaccine Uptake – July 2021 to January 2022” suggests that those who refused COVID-19 vaccination were poorer, stupider, non-English speaking foreigners. There is zero mention of the term “lockdown” or “mandate” in the publication. Revealing, no? The publication is posted on the AIRMADIP page, link here, accessed 3 July 2023.
Hulscher, N., et. al., op. cit., p 10.
Another piece of data or clarification is required is to differentiate between with having each of the vax injections and actually being defined as 'vaccinated'. Many ( if not all) jurisdictions only defined a person as being 'vaccinated' after a fortnight after the second vax injection. meaning of course that any deaths and injuries occurring within the period from receiving the first injection to a fortnight after receiving the second injection were listed as occurring to unvaccinated people. Very misleading indeed, and must be redefined.