


Inquest into the Death of Mohamed Warwar
A death in custody less than 24 hours after receipt of a Pfizer COVID-19 "vaccination" by "natural causes".

Mohamed Warwar was a 35-year-old man from South-West Sydney who had lived a chequered history struggling with drug use and mental health issues.
At about 9:20pm on the evening of Friday, 15 October 2021, Mr. Warwar was arrested by NSW Police when pulled over in a vehicle outside his parents’ house, conveyed to Bankstown Police Station and charged with three counts of possession of a prohibited drug.
By 17 October 2021, he had been transferred to the Metropolitan Remand & Reception Centre (MRRC) in Silverwater. Despite having returned a negative PCR-test result for COVID-19 at this time, Mr. Warwar was placed in a mandatory 14-day isolation cell, in accordance with the NSW Department of Communities and Justice protocols at the time.
On 22 October 2021, whilst in prison, Mr. Warwar received his first dose of the Pfizer COVID-19 “vaccine”.
By the following morning, he was dead.
As his death was in custody, a coronial inquest was undertaken in March 2024, and the findings handed down in May 2024.
The Coroner found that Mr. Warwar died from cardiac arrhythmia, with Amisulpride toxicity and myocarditis contributing factors.
In other words: from “natural causes”.
The inquest into his death examined a range of issues, including the cause of his death and how a potentially toxic level of Amisulpride (the anti-psychotic medication he was taking) could have been found in his system at post mortem.
The Court’s forensic pathologist, who conducted the autopsy following Mr. Warwar’s death, noted myocarditis in Mr. Warwar’s heart, but ultimately concluded the cause of his death was “unascertained”.1
Given that Mr. Warwar had received his first dose of a COVID-19 “vaccine” less than 24 hours before his death, his death was referred to the “Health Protection New South Wales COVID-19 Vaccine Safety Expert Panel”. The “Expert Panel” concluded Mr. Warwar’s “death was likely caused by acute cardiac arrhythmia with Amisulpride toxicity, a potential contributor to death”.
The “Expert Panel” also concluded that COVID-19 vaccine related myocarditis was unlikely, preferring to believe another viral cause of myocarditis to account for the “localised cardiac-post mortem finding was possible”.2
Given the proximity of Mr. Warwar’s “vaccination”, however, it should have been the most immediate and obvious factor explaining the myocarditis which contributed to his eventual death, so why wasn’t it?
Why wasn’t it the Pfizer “vaccination” that killed Mohamed Warwar?
Though it would appear to have been the first and most obvious avenue of inquiry, the Court-appointed experts exonerated the Pfizer “vaccination’s” role in Mr. Warwar’s death at every turn.
These attempts at doing so are outlined below:
1. It was an uncommon pattern of “vaccine”-induced myocarditis
The Court’s forensic pathologist suggested the pattern of myocarditis following Pfizer “vaccination” had not been well established in the literature, implying that Mr. Warwar’s case of “focal lymphocytic myocarditis” was less common from “vaccine”-induced myocarditis and therefore, was unlikely to have been caused by “vaccination”;
“Myocarditis can also occur following immunisation with the Pfizer COVID-19 vaccination. The typical pattern of myocarditis in these cases has not yet been well established in the literature and is thought to often be eosinophilic, though lymphocytic myocarditis has also been reported.”3
Contrary to the pathologist’s evidence, however, there is ample evidence in the literature suggesting a clear pattern of “vaccine”-induced myocarditis and it is most commonly lymphocytic myocarditis.4 In a systematic review analysing 100 publications, encompassing 73 cases of fulminant myocarditis following COVID-19 infection and 27 cases following COVID-19 vaccination, researchers found that lymphocytic myocarditis was the most common form of myocarditis following COVID-19 vaccination, with 14 out of 27 cases showing lymphocytic infiltrates.5
The pathologist's evidence was also somewhat contradictory. On the one hand, she argued that Mr. Warwar’s myocarditis was the irregular type for “vaccine”-induced cases, yet, on the other hand, suggested that there were no clear patterns for “vaccine”-induced myocarditis in the literature.
2. A viral infection could have caused the myocarditis
“The cause of the myocarditis is not clear. The most common cause for myocarditis is a viral infection.”6
The problem?
No other viral cause of myocarditis was found:
“[firstly,] focal lymphocytic myocarditis was noted in the heart. This pattern of myocarditis may be seen as a result of viral infection, though no viral infection was detected by PCR. ”7 [emphasis added]
As we know, the absence of evidence is not evidence of absence and as explained by the pathologist, post-viral myocarditis inflammatory changes could persist for some time after a viral infection was able to be detected, and therefore, a prior viral infection causing the myocarditis could not be ruled out.8
We agree, but it is essential to apply Occam's Razor correctly.
Often misunderstood to mean the simplest explanation is the correct one, it actually suggests that the simplest explanation should be the first place to look. Here, the simplest explanation should have been that the myocarditis was caused by the recent Pfizer “vaccination”, given its proximity to Mr. Warwar’s death and the extensive body of evidence demonstrating “vaccine”-induced myocarditis.
The approach taken to dismiss COVID-19 “vaccine”-induced myocarditis while readily accepting the possibility of a theorised prior viral infection without concrete evidence, sets an unfairly high bar for proving “vaccine”-induced myocarditis cases. The “Expert Panel” and Court-appointed experts unfairly demanded irrefutable proof of “vaccine”-induced myocarditis while allowing mere supposition to support a prior infectious ideology.
3. It was the Amisulpride toxicity; the “Expert Panel” already explained the cause of the myocarditis
“The overall conclusion of the expert panel was that COVID-19 vaccine related myocarditis was unlikely, but another viral cause of myocarditis to account for the localised cardiac post-mortem finding was possible. If present, this could have contributed to arrhythmia risk in the deceased. I support this view. I also support the two toxicologist expert opinions expressed that Amisulpride, even accounting for likely post-mortem effects in this case, was likely a major contributor to Mr Warwar’s death.”9
And
“[And thirdly,] even at therapeutic doses, Amisulpride may cause cardiac rhythm abnormalities including QT prolongation, bradycardia and tachycardia.”10
4. Mr. Warwar’s past drug abuse could have caused the myocarditis
“However, it is impossible to completely rule out other potential causes such as the toxic effects of Amisulpride and chronic effects of drug abuse with cocaine and methamphetamine.”11
Drawing on these conclusions of the Court’s pathologist, the Court-appointed experts and the “Expert Panel”, the Coroner found that Mr. Warwar died from a cardiac arrhythmia with Amisulpride toxicity and myocarditis being contributing factors.
The next question for the Coroner was to determine how Mr. Warwar came to have a toxic level of Amisulpride in his system beyond that which he was prescribed.
Was it “postmortem redistribution” or ingestion?
There were only two ways that the allegedly toxic level of Amisulpride could have entered Warwar’s system: through postmortem redistribution or ingestion.
These two explanations pitted the Department of Corrective Services against the experts. The former understandably wished to deflect from suggestions that Corrective Services Officers had supplied (or enabled through their administrative failings) extra Amisulpride that allegedly contributed to Mr. Warwar’s death. The latter, looking for any evidence to corroborate their hypothesis that Mr. Warwar’s death was unrelated to the Pfizer “vaccination”.
The arguments put for postmortem redistribution:
At the inquest, two of the experts described postmortem redistribution as a bit of a “magic pudding” where “strange things can happen” with the redistribution of drugs from organs to the blood, complicating an exact toxicological analysis. These experts also acknowledged that much of the redistribution occurs in the two hours immediately following death when pressed by Counsel acting on behalf of the Acting Commissioner for the Department of Corrective Services.
It was further submitted that the autopsy was carried out three days and five hours after death, so it was highly possible that the postmortem redistribution of Amisulpride could explain the apparently toxic level in his blood serum at autopsy. To support this case, it was noted by the Court’s pathologist that Mr. Warwar’s dose of Amisulpride had recently been increased prior to death:
“[Secondly,] Amisulpride was detected at an elevated level. It is unclear how much of this elevation is due to the effects of post-mortem artefact, though it is noted that the deceased’s Amisulpride dose had just been increased shortly before his death.”12
The arguments put for ingestion
When the above arguments were put to the experts at the inquest, they deflected by suggesting Mr. Warwar had experienced a relatively “normal process” of death, was transferred to the mortuary before any significant decomposition or putrefaction could occur which might have caused the elevated Amisulpride in Mr. Warwar’s blood serum at autopsy. It was suggested by the experts that the level of Amisulpride was so high, that postmortem redistribution could not account for it alone.13
The Coroner, responding to each of these arguments, made the following findings:
“I am satisfied that the toxic level of Amisulpride in Mr Warwar’s blood, postmortem, was because he had ingested a very significant amount of that substance and not because of postmortem redistribution. That finding raises the issue of how Mr Warwar, having been in custody for such a short period, could have accessed Amisulpride in a quantity necessary to cause toxicity. The evidence at inquest suggested that Mr Warwar either took the Amisulpride into custody, most likely in a balloon of some description which he swallowed, and later passed, or Mr Warwar purchased the Amisulpride from another inmate. Clear evidence was given of both the possibility and capability of these means of accessing Amisulpride in custody, including by an experienced CO [correctional officer], and no party challenged that evidence.”14 [emphasis added]
In summary, here was what was proposed.
Mohamed Warwar, a drug addict arrested for possession, was placed in an isolation cell as part of COVID-19 protocols. Though in a strict COVID-19 isolation pod, Mr. Warwar somehow obtained and ingested a dangerous excess of Amisulpride. Though completely isolated from other inmates and with minimal contact with correctional officers, he allegedly was able to smuggle, trade, or purchase additional Amisulpride. Though he had free access to an increased dosage of Amisulprisde from his doctor, Mr. Warwar either pre-empted his incarceration and smuggled an additional dosage into prison or, despite his circumstances and lack of currency whilst in prison, was able to obtain an excess dosage of Amisulpride which was a major contributor to his death.
Does any of the above make sense?
First, the suggestion that Mr. Warwar smuggled a balloon of Amisulpride, a medication he was legally prescribed, is highly doubtful. Amisulpride is not a drug of dependence and Mr. Warwar was freely prescribed this medication by his doctor, even during his brief stay in prison where his dosage was increased by 400 mg. It seems fanciful that he would have known to smuggle additional quantities into custody, especially because he would have had to have pre-empted his incarceration.
Second, the evidence presented at the inquest seemed to indicate that Mr. Warwar was completely isolated from other inmates during his brief stay in prison, as per COVID-19 protocols at the time. Therefore, he would have had limited-to-no opportunity to obtain the drug.
Third, the Coroner chastised the experienced nurses for their “errors of judgement” and “poor decisions” in their failure to respond to COs messages about Mr. Warwar’s worsening situation. The nurses were unaware Mr. Warwar was experiencing a medical emergency in his cell because they were overworked on the night he died.15 So, it would seem that the nurses were not in contact with Mr. Warwar to have provided the additional dosage that might have caused the alleged toxicity.
Fourth, the evidence presented at the inquest showed that the “knock-up calls” made by Mr. Warwar to the COs, when he was in some distress at around midnight before he died, were done remotely and did not involve the COs directly contacting or observing him, suggesting that they would have had limited opportunity to supply additional Amisulpride.
Fifth, if it was believed that Amisulpride was supplied to Mr. Warwar by COs, the nurses or other inmates, then surveillance footage might have captured this. Evidence presented to the Court revealed that surveillance footage showed both outside Mr. Warwar’s cell:

And inside his cell:

This raises an important question; how or why was the footage not examined more closely to reveal if Mr. Warwar had actually been supplied additional Amisulpride which allegedly contributed to his death?
So, it is clear from the evidence presented at the inquest that there was reduced contact between Mr. Warwar his fellow inmates, the COs and nurses, highlighting the lack of opportunity Mr. Warwar may have had to secure additional Amisulpride that contributed to the alleged Amisulpride toxicity he suffered.
These matters aside, even if we accept the opinions of the experts and the Court that Mr. Warwar took additional Amisulpride, their assessment of the toxicity of Amisulpride in his system might not be as “toxic” as believed.
The alleged Amisulpride “toxicity”
Though Amisulpride toxicity and myocarditis were acknowledged as “contributing factors” in Mr. Warwar's death, the experts clearly emphasised the role of alleged Amisulpride ingestion and toxicity, effectively downplaying myocarditis to a secondary or even negligible role. Though Mr. Warwar’s myocarditis was acknowledged several times by the experts, much of the discussion focused on the Amisulpride toxicity in causing his death. It is, therefore, relevant to evaluate this aspect of the experts’ conclusions in closer detail.
First, the allegedly “toxic” level of Amisulpride in Mr. Warwar’s body might have been overestimated by a significant degree. Research has shown that Amisulpride can redistribute from organs in the body to the blood serum, resulting in concentrations ranging from 43%-84% in days 2-8 from a patient’s admission to the mortuary to the time of a secondary postmortem sample. In the study “The Time-Dependent Post-Mortem Redistribution of Antipsychotic Drugs”, study authors showed how some individual results from the study indicated even greater postmortem redistribution exceedings 100% in some cases:
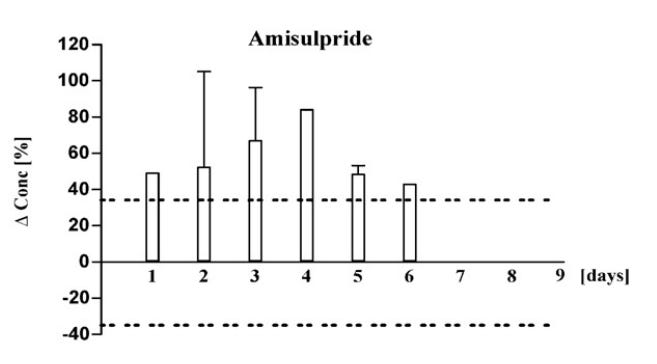
The variability highlighted by the error bars in the study’s findings shows that, while the average increase was significant, in some instances, the postmortem redistribution of Amisulpride resulted in more than a doubling of the drug concentration. In sum, it is possible that the 4.4mg/L of Amisulpride in Mr. Warwar’s blood serum could have been as low as 2.2mg/L prior to postmortem redistribution.
Second, it is relevant to question whether this concentration (possibly as low as 2.2mg/L) would have been toxic. In the Court-appointed expert’s opinion, the answer was “yes”:
“I think it’s most likely that we’re dealing with an elevated concentration, a toxic concentration, whether that was 2 milligrams or 3 milligrams or 4 milligrams, I can’t be certain but it’s likely in that range.”16 [emphasis added]
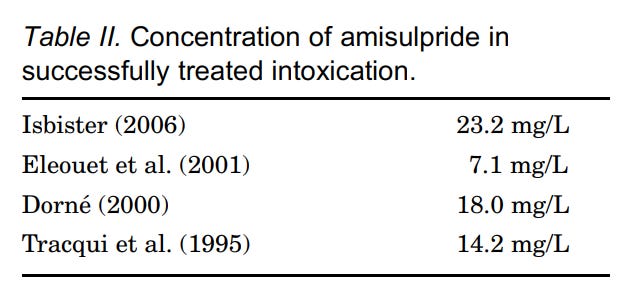
But, there are cases showing that patients could survive this allegedly “toxic” level of Amisulpride in their blood serum. The Australian study, “Fatality Due to Amisulpride Toxicity”, showed Amisulpride intoxication had been successfully treated in four patients, despite their concentration of Amisulpride vastly exceeding the 2.2-4.4mg/L in Mr. Warwar’s blood serum by a significant quantity:17
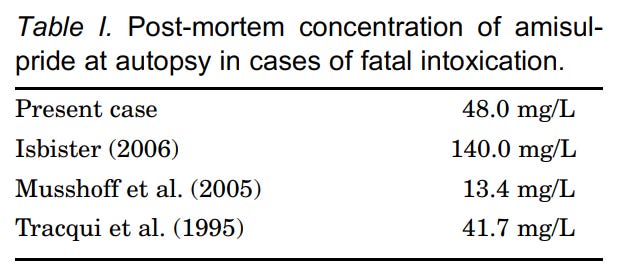
In this study, the researchers also noted the very few case reports of fatalities in the literature from Amisulpride toxicity, highlighting how only far more extreme concentrations (compared to Mr. Warwar’s) resulted in fatalities:
Third, one expert apparently misunderstood Mr. Warwar’s usage of Amisulpride and the likely impact this would have had on postmortem redistribution:
“I am confident that the issue of redistribution - did it occur? It probably did. We can’t predict the extent but it’s very unlikely, given the fact that this individual hadn’t been using the drug for an extended period of time prior to, that the - the magnitude of redistribution was such that it could conceivably have been in the therapeutic range at the time of death and then increased to 4.4 milligrams per litre at autopsy. I think that’s very unlikely.”18 [emphases added]
It was established at the inquest that Mr. Warwar was regularly using Amisulpride at a dose of 200mg nightly [“nocte”] when he was admitted to prison and that the dosage was increased to 400 mg when he was admitted to prison:

“[The prison doctor] also increased Mr Warwar’s dosage of Amisulpride (sometimes called ‘Solian’, by reason of its branding) by 400 mg daily, with the first 400 mg dose due that evening and then the next dose being 200mg the next morning.”19
So, it is possible that one of the experts miscalculated the postmortem redistribution of Amisulpride based on a misunderstanding of Mr. Warwar’s usage of the drug and how much could have been in his system.
In sum, it is possible that the quantity of postmortem redistribution for Amisulpride might have been underestimated by the experts, and that the allegedly “toxic” level in his blood serum might have been overestimated, perhaps to a significant extent. These potential errors may have led the experts and the Coroner to neglect the greater causative role of “vaccine”-induced myocarditis role in Mr. Warwar’s sudden cardiac death.
Conclusions
At the inquest into the death of Mohamed Warwar, there was a clear preference for believing anything but “vaccine”-induced myocarditis caused Mr. Warwar’s death. Though it is known that many cases of myocarditis following COVID-19 “vaccination” are neither “mild” nor “transient” for many patients, and can can also result in severe outcomes such as sudden cardiac death, Amisulpride toxicity was the main focus of the Coroner’s inquiry.20
The inquest into the death of Mohamed Warwar is emblematic of a broader problem in how we approach “vaccine”-related adverse events. It is not that we can be absolutely certain that the vaccine caused Mr. Warwar’s death, rather, it is the consistent reluctance of “experts” to consider it as a probable cause. There is an overarching systemic bias that favours any alternative explanations over the most obvious starting point; particularly when that starting point involves questioning the safety of “vaccines”.
Finally, there is the deeply unsettling possibility that Mr. Warwar, detained and in the State’s care, could have been “vaccinated” against his will. Both the Mental Health Act 2007 and the Mental Health and Cognitive Impairment Forensic Provisions Act 2020 permit using “any treatment” if it is deemed necessary for the patient’s wellbeing by a health official.
On the available evidence presented at the inquest, Mr. Warwar would have satisfied the definition under the Mental Health Act to have been considered a “mentally ill person” and warranting “treatment” “of any kind”.
We might infer that, prior to his incarceration, Mr. Warwar had decided against COVID-19 “vaccination” by his own volition. He had regular contact with health authorities and did not choose to receive the “vaccine”, even by October 2021 when approximately 85% of the NSW 16+ population was “fully vaccinated”. His decision to willingly submit to “vaccination” so soon after being imprisoned is, therefore, puzzling. If Mr. Warwar had been forcibly “vaccinated” by the State, it might explain the reluctance to acknowledge the most obvious cause of his death.
On a broader level, perhaps, there is a widespread, unspoken guilt for pushing a dangerous and failed “vaccine” that is felt in the medical community. Perhaps this guilt is the cause of the continued censorship of the reality of known “vaccine” harms and deaths like Mr. Warwar’s.
A more frightening and dangerous thought is that there might be those in the medical community who genuinely still believe in these “vaccines” and the fantasies about how they saved 20+ million lives (because some fantastical mathematical models which told them so) and they cannot possibly reconcile the idea that Mr. Warwar might simply have experienced a sudden cardiac death because of his “vaccine”-induced myocarditis.
NSW Coroner’s Court, Inquest into the death of Mohamed Warwar, paragraph 144.
Ibid., paragraph 149.
Ibid., paragraph 144.
While we acknowledge that PCR testing is not a reliable method for determining viral infection as has been addressed in our previous articles, we can generally place more confidence in a negative result than a positive one when detecting a previous viral infection. This is primarily because the high cycle thresholds used in PCR testing are more likely to amplify insignificant or non-existent viral fragments, resulting in false positives. Conversely, the likelihood of missing an actual infection (a false negative) is considerably lower.
Ibid.
Ibid.
“Lymphocytic myocarditis is the predominant pattern observed in biopsied and autopsied hearts and occurs most frequently in adolescents and young adult men who present with mild, self-limited disease.”
Marschner, C. A., Shaw, K. E., Tijmes, F. S., Fronza, M., Khullar, S., Seidman, M. A., Thavendiranathan, P., Udell, J. A., Wald, R. M., & Hanneman, K., “Myocarditis Following COVID-19 Vaccination”, Heart Failure Clinics, 19(2), 2023, 251–264. https://doi.org/10.1016/j.hfc.2022.08.012
Additionally, three cases had mixed lymphocytic and eosinophilic infiltrates, and another three cases had predominantly eosinophilic infiltrates.
Guglin, M. E., Etuk, A., Shah, C., & Ilonze, O. J., “Fulminant Myocarditis and Cardiogenic Shock Following COVID-19 Infection Versus COVID-19 Vaccination: A Systematic Literature Review”. Journal of Clinical Medicine, 12(5), 1849, 2023, https://doi.org/10.3390/jcm12051849
NSW Coroner’s Court, op. cit., paragraph 149.
Ibid., paragraph 146.
Ibid., paragraph 144.
Ibid., paragraph 146.
Ibid., paragraph 144.
Ibid., paragraph 160.
Ibid., paragraphs 167-168.
Ibid., paragraphs 192 and 207.
Ibid., paragraph 160.
Lynch, M. J., Woods, J., George, N., & Gerostamoulos, D.,“Fatality Due to Amisulpride Toxicity: A Case Report”, Medicine, Science, and the Law, 48(2), 2008 173–177. https://doi.org/10.1258/rsmmsl.48.2.173
Ibid.
Ibid., paragraph 33.
Rose et. al. suggest 2.8% mortality from myopericarditis cases following COVID-19 mRNA “vaccination” and Takata et. al. 9.6% for the same.
Rose, J., Hulscher, N., & McCullough, P. A, “Determinants of COVID-19 Vaccine-Induced Myocarditis”, Therapeutic Advances in Drug Safety, 15, 20420986241226566, 2023, https://doi.org/10.1177/20420986241226566
Takada, K., Taguchi, K., Samura, M., Igarashi, Y., Okamoto, Y., Enoki, Y., Tanikawa, K., & Matsumoto, K., “SARS-CoV-2 mRNA Vaccine-Related Myocarditis and Pericarditis: An Analysis of the Japanese Adverse Drug Event Report Database”, Journal of Infection and Chemotherapy : Official Journal of the Japan Society of Chemotherapy, 2024, https://doi.org/10.1016/j.jiac.2024.07.025
Another well-written article, thank you.
Incarceration during Emergency powers is extremely dangerous. People need to understand that once you disappear into these facilities during a SOE, your lawyer visits are cut, you are isolated, held hostage, and yes, told that you cannot see anyone until you are injected.
I have been trying to get stories from prisoners but no one is talking. They are really scared.
Fucking horrific.