
Australia's Excess Mortality Experts
Our analysis of the "thought leadership" provided by Actuaries Institute's "COVID-19 Mortality Working Group" throughout the pandemic on the nature of excess mortality and vaccine safety.

This is a long article that will be truncated by most email providers. Please read it on Substack.
Who is “Actuaries Digital”?
“Actuaries Digital” is a digital offshoot of the magazine published by the Actuaries Institute, an organisation devoted to providing a “platform for actuaries to showcase their diverse talent and thought leadership to the profession and to those in the industries served by actuaries”1.
Its “thought leadership” has become particularly prominent during the pandemic because of its “COVID-19 Mortality Working Group” (The Group), who have published semi-regular articles since early 2020 about all things COVID-19.
Though its early pandemic publications were concerned with addressing the economic and financial implications of the “pandemic” for actuaries, tracking COVID-19 cases and “vaccine” rollout for example, its attention shifted to pandemic-associated mortality, particularly once the crisis in Australian excess mortality deepened in 2022.
In a likely first for the profession, the actuaries gained notoriety from its COVID-19 “thought leadership” and have been regularly cited in the legacy media (for example here, here or here) in articles covering Australia’s excess mortality.
Politicians, likewise, have been equally willing to presume The Group’s expertise on the matter of Australia’s excess mortality, barely willing to feign their own interest in the crisis unfolding in Australian health correlating with the “vaccine” rollout.
Even Australia’s own Department of Health has deferred to The Group:

Pause for a moment to let that sink in.
Dr. Skerritt, the former head of the Therapeutic Goods Administration (TGA) (and now a Medicines Australia board member), believed it was the responsibility of a bunch of actuaries for determining “causality for things like deaths” following the largest clinical trial in human history.
Dr. Skerritt should know better, yet, he gets it so incredibly wrong.
Though it is the TGA’s responsibility to collect and evaluate information related to the benefit-risk balance of medicines in Australia2, astoundingly, even the TGA have abdicated to The Group’s “thought leadership”, in, of all places, Australia’s recent Senate inquiry into excess mortality!

Some pharmacovigilance, right?
To be fair, it’s not The Group’s fault that it has been given the loudest mouthpiece and the sole responsibility for analysing Australia’s excess mortality.
The Group humbly declares, via an honest disclaimer accompanying most of its publications:
“Articles written by the members of the Actuaries Institute are intended to provide an actuarial perspective and not a medical one. COVID-19 is a rapidly evolving health crisis and data is incomplete. Therefore, perspectives provided are themselves based on incomplete information.”3 [emphasis added]
But, as this article will show, the lines separating The Group’s actuarial and medical perspectives have become increasingly blurred.
Its main views about COVID-19 and “vaccines” could be reduced to the following:
COVID-19 “vaccines” have saved millions of lives;
The protective benefits of COVID-19 “vaccines” outweigh their allegedly very rare risks;
The TGA and other international regulatory agencies pronouncements about vaccine safety are trustworthy; and,
There is no “available evidence” that COVID-19 “vaccines” have made a “significant contribution” to excess mortality in Australia.
In this article, we refer to these assumptions as “The Paradigm”.
The Group are now regarded as the default experts for all things excess mortality in Australia.
But, if the pandemic has taught us anything, the authority of “experts” should be challenged, and their claims subjected to rigorous testing and falsification.
As our analysis in this article will show, if these are the thought-leaders in our quest to understand Australia’s excess mortality: we need to find new leaders.
2020: “The Low Mortality Year”
By any account, 2020 was a “low mortality year”, especially in comparison with the skyrocketing excess mortality of the years which have followed.
When excess mortality was negative in 2020 (that is, less deaths were recorded than were “expected”), The Group attributed the decline in total deaths from the “expected” level to the non-pharmaceutical interventions (NPIs) such as lockdowns, social distancing and face-masks. In its opinion, these all contributed to lower deaths from influenza and pneumonia, chronic respiratory illness, dementia and “other” deaths.4
“Overall the various non pharmaceutical measures to reduce the spread of COVID-19 in the period up to the end of June across Australia (lockdowns, social distancing measures, wearing of facemasks, etc) have almost certainly reduced mortality from other causes across Australia” 5 [emphasis added]
For 2020’s “Low Mortality Year”, The Group simply assumed the benefit of face masks and social distancing though, to date, the effectiveness of facemasks has neither been demonstrated in real-world settings, nor in a “gold-standard” randomised, double-blind, placebo-controlled clinical trial.6 Laughably, social distancing has now been exposed as nothing more than a thought-bubble devised in a high school science experiment which had no basis in science and “sort of just appeared”, to use Lord Pfauci’s words.
“The Science” indeed.
By suggesting NPIs had contributed to the negative excess mortality, The Group ignored the impact of the “worst flu season on record” in Australia in 2019 and the obvious role of mortality displacement in explaining 2020’s low mortality.
Mortality displacement is the situation where an increase in deaths during a particular period leads to a subsequent decrease in deaths shortly after, as the most vulnerable individuals (the elderly or those with severe health conditions) die earlier than they might have without the adverse event (the severe flu season).
Mortality displacement following the severe flu seasons in 2017 and in 2019 is clearly evident in 2018 and 2020 as shown below:

In sum, mortality displacement is the better explanation of the low mortality year in 2020, rather than the presumed effectiveness of NPIs, something which, as our analysis will show, of which The Group would have surely been aware.
2021: Excess mortality kicks off
By 2021, when excess mortality started to appear for a whole range of causes (coinciding with mass COVID-19 “vaccination”), the real effectiveness of these NPIs became apparent.
Strangely, even when Australia had virtually “Zero-COVID” in the first half of 2021, excess mortality started to really ramp up despite minimal COVID-19 transmission in the community (even using questionably accurate, hyper-sensitive PCR-testing to detect such “cases”):
And this excess mortality was driven by, among other things, increases in cardiovascular disease, which The Group acknowledged, persisted for most of 2021:
“There are very few weeks in 2021 where deaths from heart disease were lower than predicted, and only three such weeks after mid-April 2021. . . For cerebrovascular disease, actual deaths are 7% higher than predicted across 2021. . . Deaths from diabetes are . . . 7% higher over the whole of 2021.”7
The Group did not hypothesise why deaths from these causes had increased in early 2021 when there was such minimal COVID-19 prevalence in the community. Doing so would have revealed an anomaly that directly challenged The Paradigm.
The mortality increase in 2021 also had to be in excess by some magnitude to offset both the mortality improvements Australia had been making for the several decades before 2020 and decreased respiratory deaths in 2021 too.
Even more interestingly, the “almost certainty” The Group had about the protective effects of “lockdowns, social distancing measures, wearing of facemasks, etc” in protecting Australians from “COVID-19 deaths” and “non-COVID-19 deaths” disappeared in 2021. Despite the extraordinarily longer, harsher and more brutal lockdowns and other interventions which characterised the experiences of all Australians in 2021 by comparison to 2020, somehow these NPIs just didn’t cut it in 2021 for The Group.
Did we really social distance less in 2021 to explain this turnaround in Australian mortality?
Did we start ignoring those stickers on the floor telling us how far apart we had to stand?
Did we start to ignore the “how-to-wash-your-hands” cards in 2021?
Did you forget to wear your facemask in 2021, even when outside?
The Group would probably say, “yes, we did”:
“For the 65-74 years age band . . . actual deaths were lower than expected during the winter months of 2020 . . . but have been closer to expected across 2021. Perhaps this age group has become less vigilant in 2021?”8 [emphasis added]
We wonder how these NPIs were, in The Group’s opinion, so successful in 2020 for reducing Australian mortality, yet in 2021 had failed so miserably.
Once the majority of the adult population either subjected themselves or were coerced into taking the experimental “vaccine”, believing the lie that it would prevent infection and transmission of COVID-19 disease, why did these NPIs and this presumed layer of protection not lead to reduced COVID-19 and excess mortality?
The Group never addressed these obvious contradictions in its fuzzy thinking regarding Australia’s excess mortality.
Excess mortality: off the charts in 2022
By 2022, The Group hypothesised that the record increase in non-COVID-19 deaths were driven by:
The impact of COVID-19 on subsequent mortality risk;
Delays in emergency care; and
Delays in routine care.9
Most importantly for our present purposes, The Group asserted the the following were less likely to have caused the excess mortality in 2022:
Mortality displacement;
Undiagnosed COVID-19;
Mental health issues; and
Unhealthy pandemic lifestyles.10
And of course, it had nothing to do with the “vaccines”:
“[V]accination is highly unlikely to be a cause of excess mortality in 2022. Indeed, given the well-documented reduction in COVID-19 mortality risk conferred by vaccination, the 14 vaccine-caused deaths that had occurred by March 2023 are a fraction of the lives saved by vaccination.”11 [emphasis original]
The Group published the above in its April 2023 update confirming that Australia had recorded excess mortality not seen since World War Two. We will return to this point later, but remember; “mortality displacement” was considered a “less likely” cause for the excess mortality in 2022 in The Group’s opinion.
We will see how this changes later in our article.
2023: Excess mortality persists
In its April 2024 article, “Excess Mortality 5% Higher Than Pre-Pandemic Expectations for 2023” The Group offered a description of publicly available data regarding excess deaths in Australia for the year 2023. However, it stopped short of exploring the underlying reasons or causes behind these observed trends, leaving the reader with a detailed account of the data but without an analysis of the factors driving these patterns.
For instance, The Group demonstrated a complete lack of curiosity about the causes for persistently high non-COVID-19 deaths for 2023, commencing in October 2021:
“Non-COVID-19 deaths were higher than predicted for almost every week between October 2021 and mid-2023. The weeks in 2023 with lower-than-predicted non-COVID-19 deaths tend to coincide with weeks with low COVID-19 prevalence.” [emphasis added]12
Here The Group implied a relationship between excess mortality and “COVID-19 prevalence in the community,” subtly encouraging the reader to attribute the rise in excess mortality to the indirect harms of COVID-19 infection.
The suggestion, however, contradicts its analysis of 2021’s mortality:
“In the 75-84 age group . . . almost all weeks are above predicted. The presence or absence of COVID-19 at different points in the year has made little difference to the pattern of deaths relative to expected”13
It should be noted, The Group has never incorporated this type of inductive reasoning into its methodology for assessing the safety and effectiveness of COVID-19 vaccination. In The Group’s reckoning, correlation as causation is permissible only if it shows the subsequent mortality risk of COVID-19 infection: not COVID-19 “vaccine” harm. Setting aside this argument for a moment, The Group’s flawed logic prompts another crucial question: if the “fully vaccinated” still experienced “breakthrough infections” and subsequent mortality risk, then just how effective were these vaccines? At no point does The Group factor evidence of vaccine failure in its evaluation of the safety and effectiveness of the COVID-19 “vaccines”.
Yet, there is even a more substantial problem with this presumed relationship between Australia’s excess mortality and COVID-19 prevalence in the community proposed by The Group: it only started once everyone had taken the experimental shot!
Excess mortality in Australia in 2021 persisted for over six months before increases in COVID-19 mortality accelerated in Week 27:
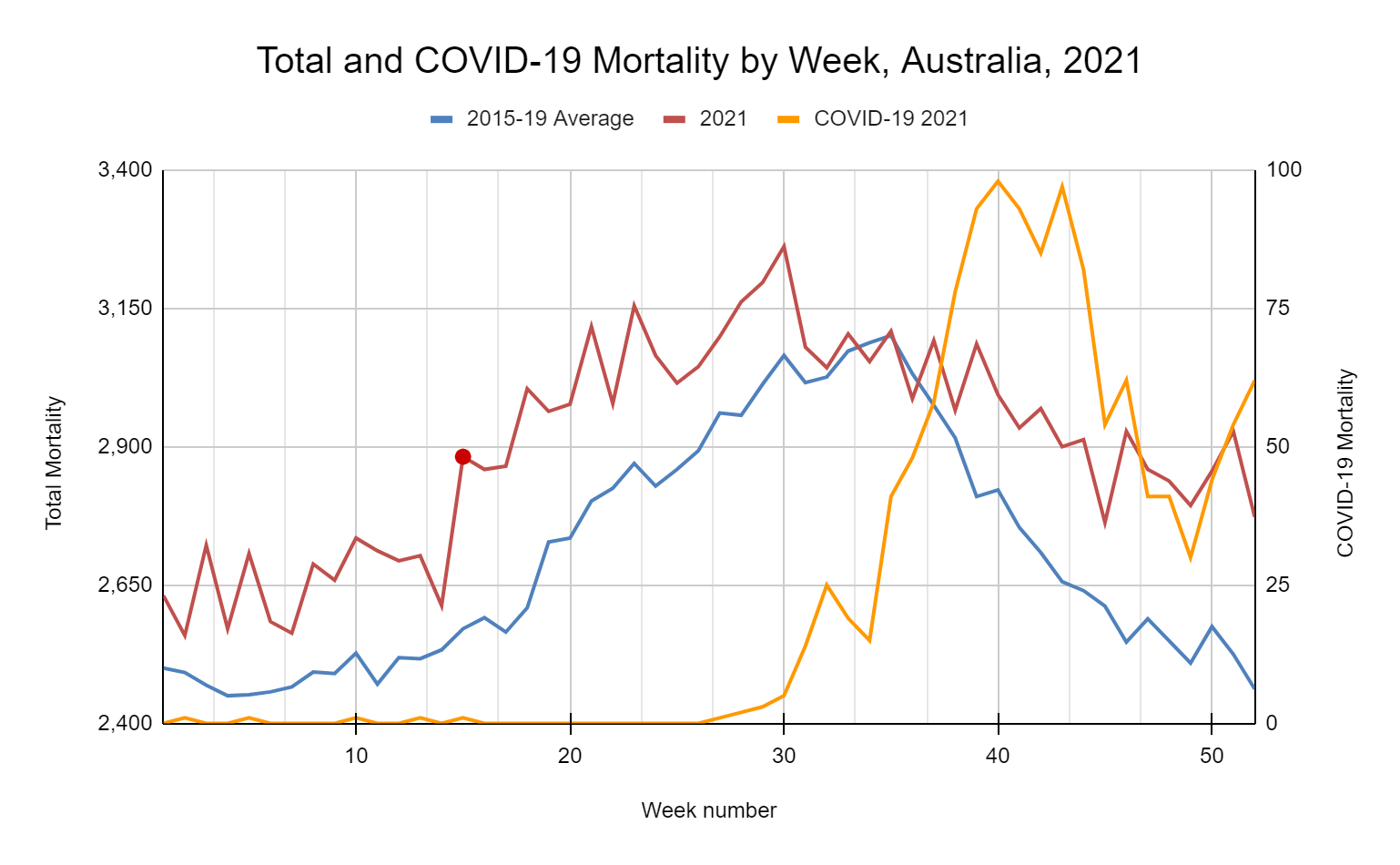
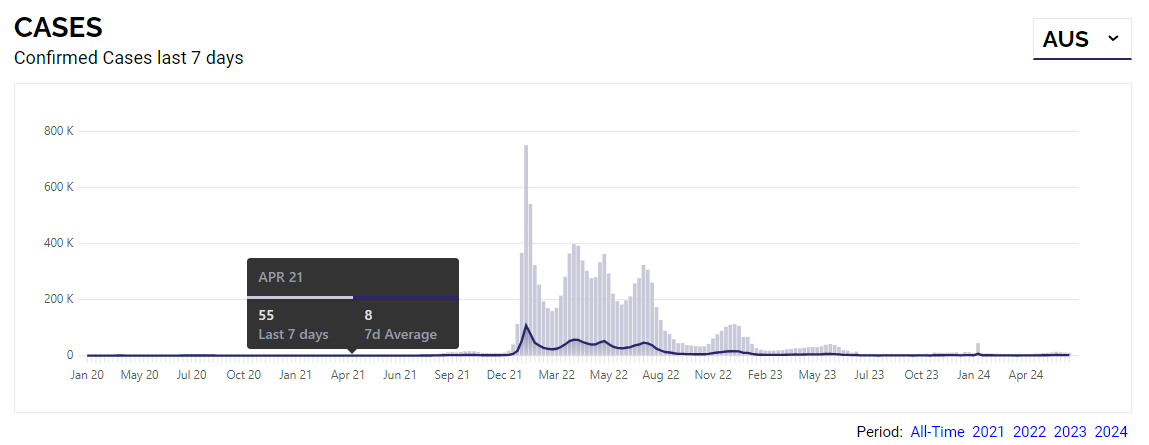
In the graph (above), note the significant escalation in mortality occurring in Week 15 (12 April 2021), coinciding with the significant escalation in the national “vaccination” rollout at this time:

In the first week of March the rolling seven day average for vaccines administered was 6,695. By the first week of April 2021, this had increased to 51,922. “Vaccine” enthusiasts will likely suggest that these data showed the “vaccines” were successful at eliminating “COVID-19 deaths” until their effectiveness waned about three months later.
Even if this interpretation were true, it could not explain why excess mortality was rising long before there were any COVID-19 “cases” in the community in all of Australia during this same period. Even using hyper-sensitive diagnostic tests like PCR, we could only find roughly a thimble-full of SARS-CoV-2 in Australia in the first week of March to the first week of April 2021:

And so, even if The Group was to pretend that COVID-19 has been the main driver of Australia’s excess mortality, they still cannot account for what was happening before COVID-19 re-entered the community and soared in the second half of 2021 in Australia.
In any event, looking for neatly fitting temporal correlations from “vaccine” administration and mortality might be misleading because acquired immune dysfunction from the “vaccines” could potentially take weeks and months to appear through down-regulation.14 In support of this proposition is the extraordinary excess mortality observed in Australia in 2022, peaking in January-February 2022, some five-six months after nearly 90% of the 16+ years population were “fully vaccinated”.15
In sum, the considerable increase in excess mortality in 2021 was driven by something other than COVID-19 and aside from the COVID-19 deaths16, “vaccines” are a likely candidate which The Group failed to properly consider.
The “Excess Mortality Inquiry” in 2024: causes and excuses for Australia’s excess mortality
Here’s where things start to turn.
When the Australian Senate announced an inquiry into Australia’s excess mortality in March 2024 (The Inquiry), as they were the trusted experts, The Group offered its “thought leadership” once more.
In its submission, The Group surprisingly upgraded “mortality displacement” to the status of a major cause of Australia’s excess mortality, having only deemed it a “less likely” cause as early as April 2023. The reasons for this upgrade could be described as “murky” at best:
“While we have not studied this phenomenon in any detail, we consider that mortality displacement (in addition to COVID-19 prevalence) represents a reasonable explanation of the timing of peak excess mortality”17 [emphasis added]
In further fuzzy thinking from The Group, for reasons neither studied “in any detail” nor explained, mortality displacement from “low early pandemic mortality” resulted in Australia’s record excess mortality in 2022.
There are two major flaws in this thinking.
First, Australia’s low early pandemic mortality was very different from 2020 to 2021. The “low mortality” of 2020 was the result, as addressed previously, of negative mortality displacement following the “worst flu season on record” in Australia. It was not because of pseudoscientific NPIs with wishfully thought endpoints like “lower COVID-19 prevalence”. Though 2021 commenced in much the same way with virtually “Zero-COVID” in the Australian community, Australia still recorded more than 10,660 excess deaths in 2021.18 2021 was not a “low mortality year” and could not, therefore, contribute to negative mortality displacement in the ways claimed by The Group.
Second, it is expected that mortality displacement should resolve over a much shorter period of time than is required to explain Australia’s persistent excess mortality. Five years into the pandemic, Australia is now into its fourth year of record-breaking, expert-baffling excess mortality which shows no signs of abating. It should be readily apparent to any objective observer that mortality displacement cannot explain the scale or persistence of excess mortality in Australia.
The Group’s analysis then shifted to the question of COVID-19 “vaccine” harm in explaining excess mortality:
“We are aware that excess mortality has been attributed to COVID-19 vaccines by some, but we are unable to identify evidence to support this claim and our view is that adverse impacts of COVID-19 vaccines are unlikely to be a significant contributing factor. Rather our view is quite the reverse: COVID-19 vaccines have significantly reduced excess mortality.”19 [emphasis original]
The above represents either The Group’s dishonesty or extraordinary lack of curiosity. The Group does not provide evidence of its efforts to “identify evidence” inviting the reader to assume that there is no evidence to support the claim that the COVID-19 “vaccines” were a significant contributing factor in Australia’s excess mortality, when there is clinical and empirical evidence of “vaccine” harm and its role in causing Australia’s excess mortality.20
The Group’s faith in the healing power of the “vaccine” relies on eight important misdirections; each failing to counter the clear evidence that the “vaccines” have caused and are causing Australia’s record excess mortality:
1. Appeal to authority
Remember the same TGA who abdicated their authority to the “expertise” of The Group earlier in the article? Here The Group deflects back to the TGA:

Note the contradiction. The Group trusts the TGA to “link” just the 14 deaths to the “vaccines” from the 1,004 reports received to affirm their safety, yet, admits “The TGA does not make formal determinations of cause of death for individuals” because “that is the role of treating medical practitioners”. By The Group’s logic, we should trust the 1,004 reports of death from the medical practitioners and coroners because it is not within the TGA’s remit to make determinations of the causes of death for individuals.
The Group is also seemingly unaware of the Australian underreporting rate, estimated by some to be above 99%.21 So, despite the TGA’s Database of Adverse Event Notifications (DAEN) providing valuable and objective empirical evidence of harms from “vaccines”, these 1,004 reports of death are likely just the tip of the iceberg.
2. A flawed conception of the nature of “vaccine” harm
An erroneous assumption that all “vaccine” deaths must immediately follow “vaccine”-administration:

As Wilson Sy points out, “contemporaneous correlation should not be expected because there is normally a time-lag between medication (the cause) and its effects . . . [t]he initial doses of injection may have weakened the immune system of the recipients to make them more vulnerable to subsequent challenges introduced e.g. by the boosters, a phenomenon also known as “antibody dependent enhancement” of disease”.22
The Group also incorrectly suggests that excess mortality did not correspond with the timing or shape of excess mortality, which is also partly incorrect. The most extraordinary months of excess mortality in Australia were in the months January-February 2022 and again in June-July 2022, coinciding with mass booster vaccination at these times (3rd and 4th or “winter dose” respectively):

3. Straw man fallacy
By taking down an argument no one had made, The Group assures us that the allegedly rare and mild cases of myocarditis following “vaccination” were not directly contributing to excess mortality:
Focusing on myocarditis-related deaths is a straw man argument. It diverts attention from the broader array of adverse events linked to the “vaccines”. By framing the issue solely around this condition, the argument overlooks the broader risks, reducing the complex debate to a single, more easily dismissible point.
But, even if we accept this aspect of The Group’s defence of the “vaccines”, it is still problematic.
First, it is incorrect. At the recent Senate Inquiry into Australia’s Excess Mortality, the ABS’s Director for its Health and Vital Statistics Section, Lauren Moran spoke about increases in myocarditis, compared with pre-vaccination years, as an associated cause of death for 2022 (with it unknown as to whether COVID-19 or “vaccination” was driving this trend):

…

Second, The Group’s argument glosses over concerns about the long-term impacts myocarditis and pericarditis could have on individuals who develop them after “vaccination”. Myocarditis, while rarely fatal on its own, can lead to a cascade of other serious health issues that may ultimately result in death. These can include arrhythmias, myocardial infarction, sudden cardiac death, or conditions broadly categorised as “sudden adult death syndrome” (SADS). All of these conditions might fall under the broad category of “heart disease”, which, as The Group had acknowledged in 2022 had been a driver of excess mortality since April 2021:
“There [were] very few weeks in 2021 where deaths from heart disease were lower than predicted, and only three such weeks after mid-April 2021”23
It is also likely that the low numbers of myocarditis or pericarditis deaths may not even reveal the full picture. To date, Australia’s DAEN has received over 12,000 reports of “cardiac disorders” for a single suspected medicine (the original Pfizer COVID-19 “vaccine”), likely revealing the potential for continued serious cardiac conditions to impact Australia’s mortality for the future:

Recalling of course, that because of the underreporting rate, these numbers are plausibly significantly higher than these reports reveal.
Finally, we are aware of many deaths from myocarditis in Australia in “vaccinated” individuals such as YouTuber “Pretty Pastel Please”, South Australian woman Hayley Beadman, and young Melbourne woman Natalie Boyce to name a few, demonstrating that the “vaccine” can actually cause fatal myocarditis and pericarditis too.
4. Further appeals to authority and straw man fallacies
Once again The Group returns to the authority of the TGA and “other international medicines regulator[s]” to defend the “vaccines”, layering this defence with the straw man argument that “vaccine”-driven excess mortality could only result from increases in ischaemic heart disease:

There are several problems with this proposition.
First, the TGA has admitted that they do not and can not determine causality for all the COVID-19 “vaccine” adverse event reports they have received, rendering as meaningless this aspect of The Group’s argument.
Second, the argument relies on an appeal to authority one more (TGA and “international medicines regulator”) and misrepresents the issue by focusing solely on ischaemic heart disease, creating a straw man because “vaccine”-related excess mortality is not limited to ischaemic heart disease alone.
Third, ischaemic heart disease has been in excess since the “vaccination” rollout:
“More than 10,200 Australians died of ischemic [sic] heart disease in the first eight months of 2022 – that is about 17 per cent higher than would be expected in a normal year.”24
Third, many of the long-term safety studies by the “sponsors” have not yet concluded for these “frail” cohorts like those with ischaemic heart disease. Here is the “Nonclinical Summary and Recommendations” for Moderna’s “Spikevax” released under Freedom of Information (FOI) request by the TGA, showing that Moderna had pledged to, “to the extent that it [was] feasible”, monitor the safety concern for “frail subjects” using their product which does not conclude until April 2025:

And in Pfizer’s Australian Public Assessment Report by the TGA, those with “cardiovascular disorders” were excluded from the pharmacovigilance and risk management plan for its “vaccine”:

Fourth, neither The Group nor the TGA has provided any evidence that the TGA is actually even investigating a causal link between COVID-19 “vaccines” and ischaemic heart disease. We do, however, know that these results have been published in the academic literature.25
These matters aside, once again The Group has committed the straw man fallacy. Its insistence on debunking the proposed link between ischaemic heart disease and the “vaccines” diverts attention from the plethora of other serious adverse events linked to the “vaccines” as we have addressed so far in this and other articles. It also does not actually address the existence of significant excess mortality in the pandemic period from ischaemic heart disease.
5. Deflection

The analysis here is simply wrong. Statistically significant increases in mortality (compared against a 2015-2019 baseline average) are evident for the following cohorts:
2021:
55–64 years cohort 14,374 deaths (an excess of 268 deaths)
2022:
45-54 years cohort 3,593 deaths (an excess of 371 deaths)
55-64 years cohort 15,430 deaths (an excess of 1,324 deaths)
The Group’s argument is also misleading. By implying that “vaccine”-related harms would manifest equally across all age groups, it ignores the reality that the elderly population, who already face higher mortality risks, would naturally be more vulnerable to any additional stressors, including potential “vaccine”-related complications. The implication that younger age groups should exhibit a similar scale of excess mortality deflects from the issue; the alarming increase in deaths in the 65+ years cohort.
6. Red herring
The Group commits a classic red herring by attempting to shift the focus away from the real concerns of “vaccine” harm, which are not about “unidentified” risks but rather the underreported and ignored risks:

The Group’s argument is also deeply misleading. The claim that all vaccine batches are identical across the globe ignores the well-documented fact that different vaccine batches exist.26 Some batches have been shown to have significantly higher rates of adverse reactions and deaths than others. This information is not hidden, but publicly available, making this omission by The Group either an act of wilful ignorance or deliberate deception.
And what of the “extreme unlikelihood that there remains a significant unidentified risk of death from the COVID-19 ‘vaccines’”?
Who had ever maintained the risk was unidentified?
The concern we and many others have raised is not about unidentified risks but known, underreported and ignored risks (particularly with specific batches) and the broader implications of ongoing “vaccination” propaganda for a whole range of identified causes. The Group’s framing of this point is either completely disingenuous or a reflection of its failure to fully engage with the evidence at hand.
By focusing on the unlikely prospect of an entirely unknown danger, The Group diverts attention from the actual, documented adverse events that have already been identified and acknowledged. The Group falsely implies critics are making baseless claims about “hidden risks”, when the actual issue is about transparency and recognition of known risks that are being downplayed or ignored.
7. Appeal to ignorance

This statement is a clear appeal to ignorance. By claiming, “we have not been able to find an obvious statistical relationship suggesting that COVID-19 vaccinations caused excess mortality”, The Group are implying that because they “cannot find” the evidence, it must not exist. However, as has been demonstrated by various studies and documented cases, there is plenty of evidence suggesting a relationship between “vaccination” and excess mortality.
When The Group states they “cannot find it”, they are either admitting that they have found such evidence but disagree with it, or that they haven’t found it at all, which is troubling because this evidence is publicly available.
The Group’s statement is also misleading, because the ABS does not include vaccination status in its reporting of deaths. To date, neither the ABS nor The Group have published any analyses using the AIRMADIP (Australian Immunisation Register Multi-Agency Data Integration Project) data, which could provide insights confirming the “vaccination” status (doses, batch, brand, timing) of the deceased in Australia. As The Group acknowledges, neither an “exhaustive analysis” nor any sufficient analysis, has been conducted to verify its claim.
Therefore, The Group’s inability to find evidence is not proof of its absence but rather a reflection of either intentional omission or insufficient investigation, prompting the question once again: why are they the trusted “experts”?
8. One final appeal to authority

In the final defence of the “vaccines”, The Group makes an audacious appeal to one of the most seriously flawed “studies” to purport Australia somehow avoided 50,000 extra deaths because of the saving power of the “vaccines”.
With only one citation for this study to date, it appears serious researchers are not keen on touching the study with a ten-foot pole.
The data used in the study to make that claim about 50,000 saved deaths came from the seriously crippled NSW Health Weekly Surveillance Reports. Here were some of the highlights of the methodology used in these reports:
Incidental hospitalisations with COVID-19 were counted as “COVID-19 hospitalisations” irrespective of whether COVID-19 had anything to do with a patient’s hospitalisation;
ICU-admitted COVID-19 patients were double-counted as “COVID-19 hospitalised patients”;
“COVID-19 deaths” were recorded so even if COVID-19 was not the primary cause;27
Which led reporters to somehow find:
More weekly “COVID-19 deaths” in NSW than Australian weekly “COVID-19 deaths” (for the same weeks) on six separate occasions in 2022; and,
Approximately 2,000 more “COVID-19 deaths” in NSW than the ABS had for NSW in 2022.
It goes without saying that the flawed methodology applied by NSW Health exaggerated the severity of an alleged “pandemic” of COVID-19, enabling support for lockdowns, coercive vaccination mandates and a range of all other illiberal interventions in our daily lives.
We addressed these in our series of articles “What Happened with COVID-19 in NSW in 2022” and Letters from Australia has also written a brutal takedown of the above study here.
So, in defending the “vaccine’s” role in excess mortality, why would The Group appeal to the authority of this study? We can only assume it is confirmation bias. The Group has not provided any rigorous analysis of the study’s claims and it appears as though the logic of integrating this study into its defence of the “vaccines” could be crudely summed as “not the ‘vaccine’ because study said so”.
Reflection
Our analysis has shown that The Group is simply a “puzzle-solver”:
Puzzle-solvers expect to have a reasonable chance of solving a puzzle;
The puzzle itself and its methods of solution will have a high degree of familiarity;
The puzzle-solver does not enter uncharted territory, because puzzles and their solutions are pre-set and straightforward;
Australia’s excess mortality, to The Group, has been like solving a puzzle:
A huge piece of the puzzle says “COVID-19”; and,
Some smaller pieces say “after effects of COVID-19” and “delayed emergency care” or “delays in routine care”.
For some strange reason though, the puzzle can’t be solved; the pieces don’t fit neatly together and the emerging picture is distorted.
So The Group opens a different puzzle-box and picks out a piece called “mortality displacement” and another “undiagnosed COVID” and tries to squish those pieces into the half-completed puzzle. Even though The Group knows it took these pieces from a different puzzle box, it convinces itself that these pieces should really go into this new puzzle.
It requires some force to stick the pieces together, but The Group makes it work and convinces itself the puzzle is “solved”.
The Group takes a photo of its solved puzzle.
The Group uploads the photo to its social media.
The Group publishes it on its webpage.
Bureaucrats hear about the solved puzzle and tell their superiors about it, and all and sundry get to tell the story about how the puzzle was solved!
But there’s still a piece left in the box.

Even The Group can see this puzzle piece, but fail to recognise its importance:

But, some notice the anomaly; they can see that the picture doesn’t make any sense. The colours and the image and the pieces do not fit together in any meaningful way.
“Antivaxxer!” the NPCs retort.
“Conspiracy theorist!” the fetid Senator Ayres shouts.
“Science Denier!” cries Albo.
“But the picture doesn’t make any sense”, those who see the anomaly say.
The Group is doing its best to make these pieces fit, but many are starting to see how the Paradigm cannot solve this particularly worrying puzzle and a revolutionary shift in thinking is needed.
Conclusion
The convenient narratives being fed to us cannot account for the scale and persistence of excess mortality Australia has recorded since the largest clinical trial in human history commenced.
The pandemic has shown us that expertise must be earned, not assumed. The Group’s rise to prominence has been driven more by the absence of other voices than by any proven superiority in understanding the causes of excess mortality. Unconditional trust in these “experts” is dangerous, especially when they fail to provide clear, consistent answers or fully acknowledge the limitations of their own data and methods.
Final thoughts
As they are busily preparing us for the next pandemic, we encourage you all to write to your elected officials and demand a proper inquiry that is truly independent, transparent, and open to all possibilities; one that doesn’t shy away from asking the hard questions, even when the answers might be uncomfortable.
Do the same with your family, friends and colleagues.
Re-engage with them.
Ask them why they stopped taking the “vaccines” and when they finally felt safe again.
Ask them how, why and when that changed.
Inquire about the sources they used to make this decision.
Ask them what they would do if they try to bring in lockdowns again.
Ask them how they would act if “vaccination” mandates were reintroduced.
Importantly, listen to what they have to say but do not self-censor.
We can’t beat the censorship of Big Tech.
We can’t rely on the legacy media to honestly and openly admit the truth.
Our views need to be shared beyond the closed community that is Substack.
That is, if we want the Paradigm to shift.
Actuaries Digital, “About Us”, https://www.actuaries.digital/about-us/, accessed 18 June 2024.
The Department of Health and Aged Care, Pharmacovigilance responsibilities of medicine sponsors”, https://www.tga.gov.au/resources/resource/guidance/pharmacovigilance-responsibilities-medicine-sponsors, accessed 8 July 2024.
Actuaries Digital, “COVID-19 Articles”, https://www.actuaries.asn.au/microsites/pandemics-resource-centre/covid-19-articles, accessed 24 June 2024.
We understand this could refer to the many other causes of death not in the “leading causes of death” calculation and/or a substantial number, as to be expected in early cause of death reporting, to be from “unknown” causes (ICD-10 R00-R99) which may be revised and reassigned to “known” causes in subsequent causes of death “revisions”.
Actuaries Digital, “Update on Mortality in Australia”, 16 October 2020, https://www.actuaries.digital/2020/10/16/update-on-mortality-in-australia/, accessed 20 June 2024.
Writing in May 2020, the Group assured us that some hamsters were likely better off for wearing facemasks though: see here.
Actuaries Digital, “COVID-19: Deaths in 2021 Were around 1%, or 2,000 More than Expected, Had There Been No Pandemic”, https://www.actuaries.digital/2022/04/05/covid-19-deaths-in-2021-were-around-1-or-2000-more-than-expected-had-there-been-no-pandemic/, accessed 30 June 2024.
Actuaries Digital, “How COVID-19 has affected Mortality and Morbidity in 2020 & 2021”, https://web.archive.org/web/20221109042850/https://www.actuaries.asn.au/Library/Opinion/2022/ResearchNoteno4.pdf, p. 27, accessed 9 July 2024.
Actuaries Digital, “COVID-19 Mortality Working Group: Confirmation of 20,000 Excess Deaths for 2022 in Australia”, https://www.actuaries.digital/2023/04/06/covid-19-mortality-working-group-confirmation-of-20000-excess-deaths-for-2022-in-australia/, accessed 30 June 2024.
Ibid.
Ibid.
Actuaries Digital, “Excess Mortality 5% Higher Than Pre-Pandemic Expectations for 2023”, https://www.actuaries.digital/2024/04/05/excess-mortality-5-higher-than-pre-pandemic-expectations-for-2023/, accessed 2 July 2024.
Actuaries Digital, “How COVID-19 has affected Mortality and Morbidity in 2020 & 2021”, https://web.archive.org/web/20221109042850/https://www.actuaries.asn.au/Library/Opinion/2022/ResearchNoteno4.pdf, p. 27, accessed 9 July 2024.
Sy, W., “Simpson's Paradox in the Correlations between Excess Mortality and COVID-19 Injections: A Case Study of Iatrogenic Pandemic for Elderly Australians”, Medical and Clinical Research, Vol. 8, 7 ,June, 2023, p. 7.
The expansion of the booster program at this time is likely to have been a major contributor to the excess mortality observed with more immediate effects shown (< 6 weeks).
Accurately coding a COVID-19 death presents its own problems as we addressed in our article here https://shiftedparadigms.substack.com/p/the-underlying-truth-with-covid-19. It is entirely possible that an adverse event to COVID-19 “vaccine” causing death could have been a death that was “clinically compatible” with COVID-19 and would, therefore, distort the true picture about the COVID-19 versus non-COVID-19 deaths.
Actuaries Institute, Submission to Senate Community Affairs References Committee Inquiry into Excess Mortality, https://www.actuaries.asn.au/Library/Submissions/LifeInsuranceWealth/2024/240522COVIDSUB.pdf, accessed 3 September 2024.
The ABS’s “Provisional Mortality Statistics, Jan 2024” shows 171,819 total deaths for 2021, in excess of the 2015-19 average of 161,159: a difference of 10,660 deaths.
Actuaries Institute, op. cit.
For a few Australian examples see:
Sy, W., “Australian COVID-19 Pandemic: A Bradford Hill Analysis of Iatrogenic Excess Mortality”, Journal of Clinical & Experimental Immunology, 8 (2), 542-556 https://doi.org/10.33140/jcei.08.02.01 AND Sy, W., “Simpson's Paradox in the Correlations between Excess Mortality and COVID-19 Injections: A Case Study of Iatrogenic Pandemic for Elderly Australians”, Medical and Clinical Research, 8(7) ,June, 2023, p. 7.
Rhodes, P., & Parry, P. (2024). “Gene-Based COVID-19 Vaccines: Australian Perspectives in a Corporate and Global Context”, Pathology, Research and Practice, 253, 155030. https://doi.org/10.1016/j.prp.2023.155030
Turni, C., and Lefringhausen, A., “COVID-19 Vaccines – An Australian Review”, Journal of Clinical & Experimental Immunology, 7(3), 2022, 491-508.
For a global example see:
Aarstad, J., and Kvitastein, O.A, “Is There a Link between the 2021 COVID-19 Vaccination Uptake in Europe and 2022 Excess All-Cause Mortality?”, Asian Pacific Journal of Health Sciences, 2023, https://doi.org/10.21276/apjhs.2023.10.1.6
Li, R., Curtis, K., Zaidi, S. T. R., Van, C., Thomson, A., and Castelino, R., “Prevalence, Characteristics, and Reporting of Adverse Drug Reactions in an Australian Hospital: A Retrospective Review of Hospital Admissions Due to Adverse Drug Reactions”, Expert Opinion on Drug Safety, 2021, 20(10), 1267–1274. https://doi.org/10.1080/14740338.2021.1938539
Sy, W., “Australian COVID-19 Pandemic: A Bradford Hill Analysis of Iatrogenic Excess Mortality”, Journal of Clinical & Experimental Immunology, 8 (2), p. 549.
See also “FOI 4205 – Reports of death in people who have been vaccinated with a COVID-19 vaccine” revealing that the majority of adverse events to “vaccination” causing death occurred six weeks following “vaccination”.
Actuaries Digital, “COVID-19: Deaths in 2021 Were around 1%, or 2,000 More than Expected, Had There Been No Pandemic”, https://www.actuaries.digital/2022/04/05/covid-19-deaths-in-2021-were-around-1-or-2000-more-than-expected-had-there-been-no-pandemic/, accessed 3 September 2024.
Aisha Dow, “Fatal heart attacks have surged in Australia. Here’s why”, https://www.smh.com.au/national/fatal-heart-attacks-have-surged-in-australia-here-s-why-20230117-p5cd22.html
In a study comprising over 103,000 reported adverse events, researchers investigated cardiovascular side effects related to COVID-19 “vaccines”. They focused on events such as tachycardia, hypertension, and serious conditions like acute myocardial infarction and cardiac arrest. Through disproportionality analysis, a method used to detect whether certain side effects occurred more frequently than expected, the researchers found signals linking these cardiovascular events to the “vaccines”, particularly in individuals aged over 75 years. The study highlighted a very real risk for specific populations, particularly the elderly, who may be prone to cardiovascular events post-vaccination.
Jeet Kaur, R., Dutta, S., Charan, J., Bhardwaj, P., Tandon, A., Yadav, D., Islam, S., and Haque, M., “Cardiovascular Adverse Events Reported from COVID-19 Vaccines: A Study Based on WHO Database”, International Journal of General Medicine, 14, 2021, 3909-3927.
Manniche V., Schmeling M., Gilthorpe and J. D., Hansen P. R., “Reports of Batch-Dependent Suspected Adverse Events of the BNT162b2 mRNA COVID-19 Vaccine: Comparison of Results from Denmark and Sweden”, Medicina. 2024; 60(8):1343. https://doi.org/10.3390/medicina60081343
In a now deleted excerpt from a NSW Health webpage “COVID-19 surveillance report data sources and methodology”, it is explained: “For 2020 through 2021, NSW Health categorised deaths as COVID-19 deaths if they met the definition in Communicable Diseases Network of Australia’s (CDNA) COVID-19 National Guidelines for Public Health Units. As per the CDNA definition, deaths were considered COVID-19 deaths for surveillance purposes if the person died with COVID-19, not necessarily because COVID-19 was the cause of death.”
Thanks for putting this together. I agree with the comments on 2020. It was no more than one standard deviation from the trend on previous years. There will have been a small effect due to border closures and minimal influenza. You are right 2019 was a worse than normal influenza year in many states of Australia. We typically expect below trend the following year. The small deficit has been used to try to explain away the huge jump >3SD in 2021. There is no evidence to support that non-pharmacological measures like masks, hand washing and social distancing reduced the deaths in 2020 and stopped reducing them in 2021.
A devastating takedown.
>It requires some force to stick the pieces together
Denial. People cannot admit that they killed their children. They also know that there is no fixing what has happened. There is no way to make this better.
The SPARS document says that when 'it comes out' the vaccine dead and injured will be framed as the 'heroes of the pandemic' but I do not think that will ever happen. I think they have run out the clock and they are pivoting to war.
Thanks again for your excellent, excellent writing.